

Population Pharmacokinetics of Tenofovir in Pregnant and Postpartum Women Using Tenofovir Disoproxil Fumarate
- PMID: 33318014
- PMCID: PMC8092509
- DOI: 10.1128/AAC.02168-20
Population Pharmacokinetics of Tenofovir in Pregnant and Postpartum Women Using Tenofovir Disoproxil Fumarate
Abstract
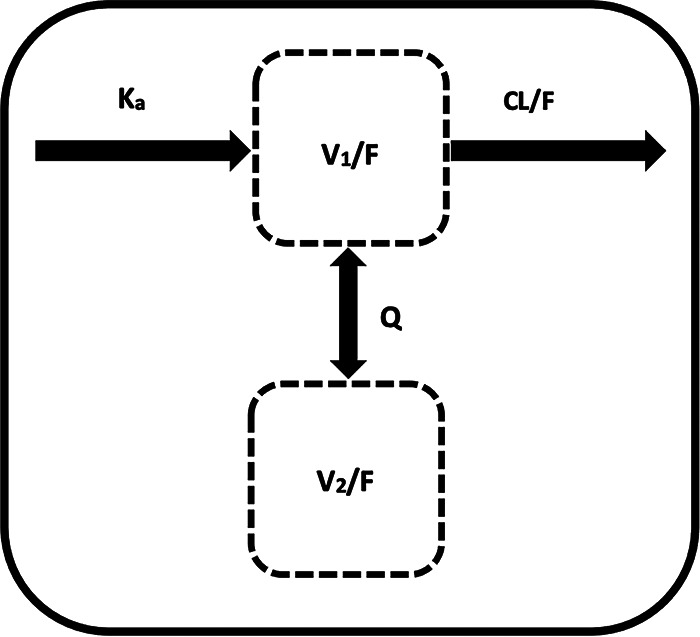
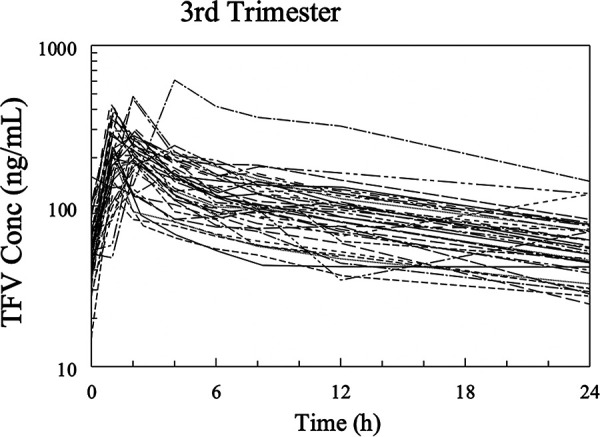
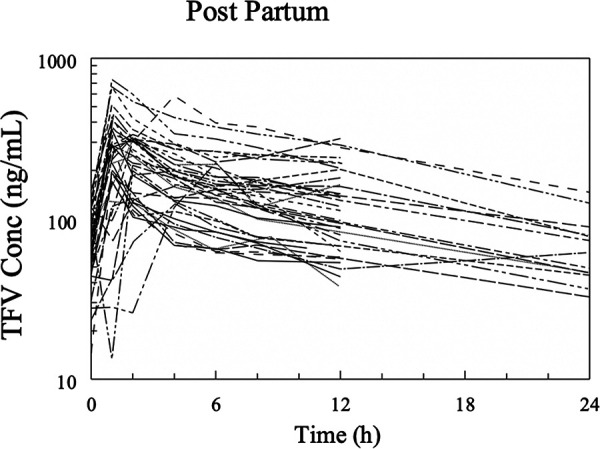
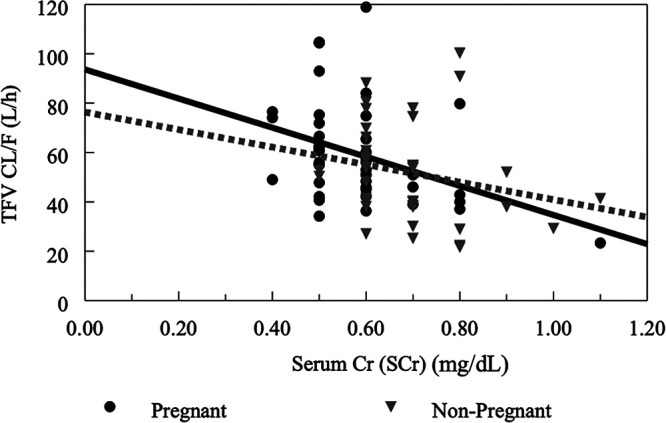
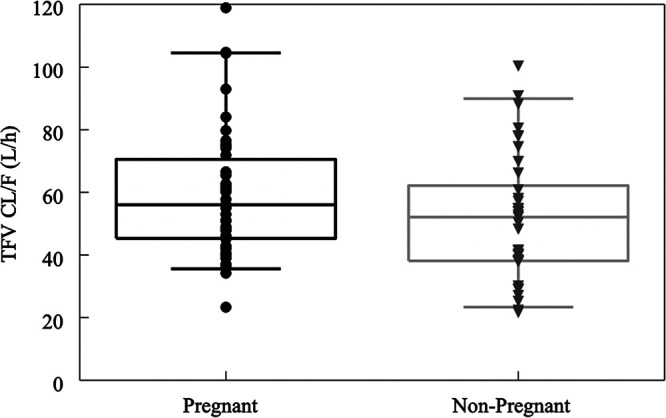
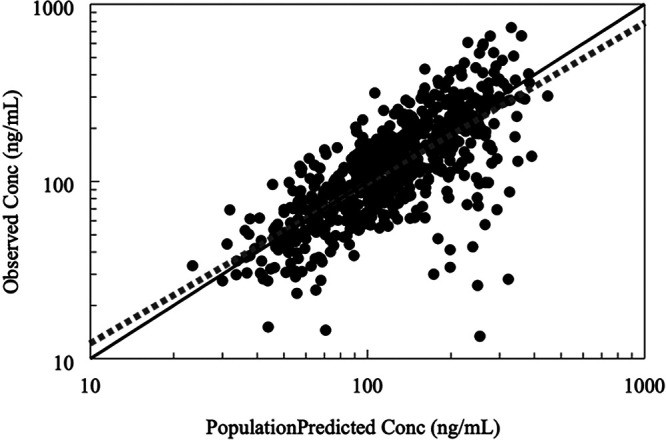
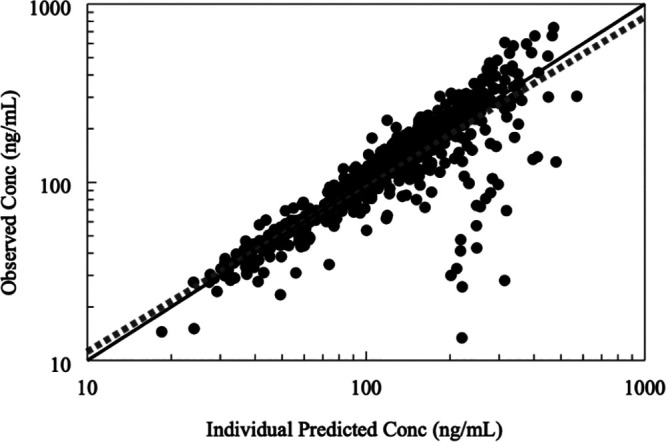
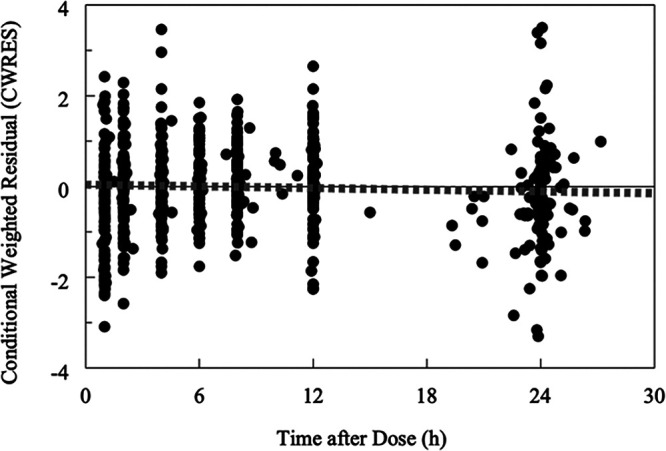
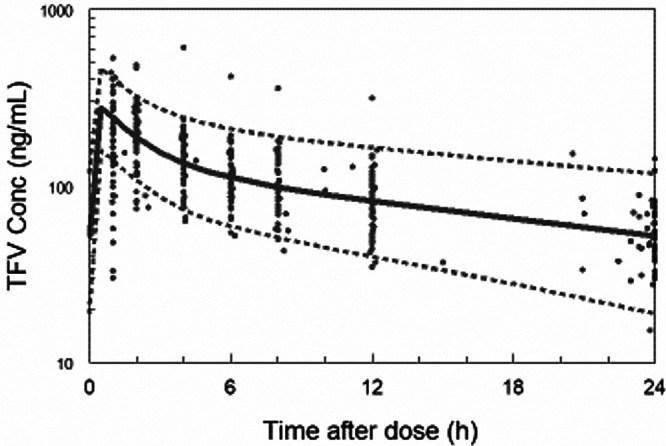
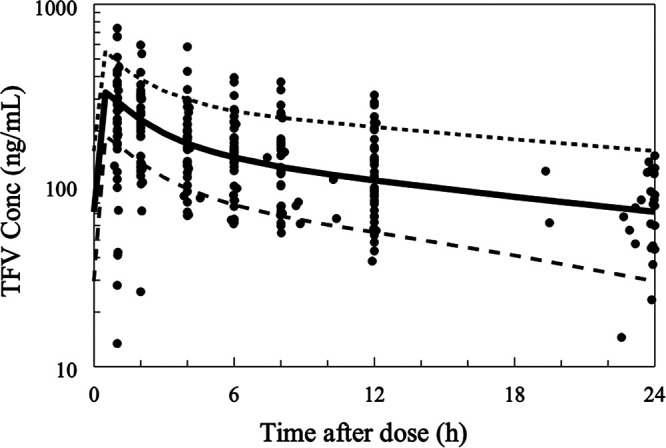
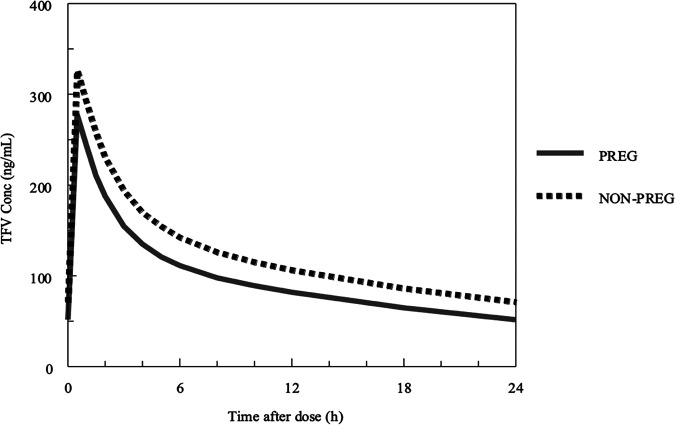
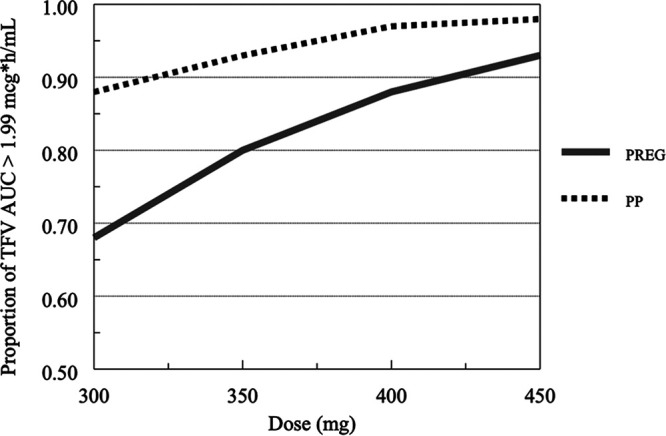
Pharmacokinetics of drugs can be affected by physiologic changes during pregnancy. Our aim was to assess the influence of covariates on tenofovir (TFV) pharmacokinetics in pregnant and postpartum women receiving tenofovir disoproxil fumarate (TDF). Population pharmacokinetic parameter estimates and the influence of covariates were assessed using nonlinear mixed-effects modeling (NONMEM 7.4). Forty-six women had intensive pharmacokinetic evaluations during the second and third trimesters of pregnancy, with another evaluation postpartum. A two-compartment pharmacokinetic model with allometric scaling for body weight and first-order absorption best described the tenofovir plasma concentration data. Apparent oral clearance (CL/F) and volume of distribution at steady state (Vss/F) were increased during pregnancy. Weight, serum creatinine (SCr), pregnancy, albumin, and age were associated with TFV CL/F during univariate assessment, but in the multivariate analysis, changes in CL/F and Vss/F were only associated with increased body weight and enhanced renal function. Due to greater weight and lower SCr during pregnancy, CL/F was 28% higher during pregnancy than postpartum. In the final model, CL/F (liters per hour) was described as 2.07 × (SCr/0.6)0.65 × weight0.75, with a low between-subject variability (BSV) of 24%. The probability of target attainment (proportion exceeding area under the concentration-time curve of >1.99 μg·h/ml, the 10th percentile of average TFV exposure for nonpregnant historical controls) was 68%, 80%, 87%, and 93% above the target with 300 mg, 350 mg, 400 mg, and 450 mg of TDF, respectively, during pregnancy and 88%, 92%, 96%, and 98% above the target with same doses in postpartum women. Dose adjustment of TDF during pregnancy is not generally warranted, but any modification should be based on weight and renal function. (This study has been registered at ClinicalTrials.gov under identifier NCT00042289.).
Keywords: AIDS; HIV; TDF; population pharmacokinetics; postpartum; pregnancy; tenofovir; tenofovir disoproxil fumarate.
Copyright © 2021 American Society for Microbiology.
Figures
References
-
- Panel on Treatment of Pregnant Women with HIV Infection and Prevention of Perinatal Transmission. 2020. Recommendations for the use of antiretroviral drugs in pregnant women with HIV infection, and interventions to reduce perinatal HIV transmission in the United States–August 26. https://clinicalinfo.hiv.gov/sites/default/files/guidelines/documents/Pe.... Accessed 18 September 2020.
-
- Gilead. 2004. TRUVADA (emtricitabine and tenofovir disoproxil fumarate) tablets for oral use—drug label. https://www.gilead.com/%7E/media/files/pdfs/medicines/hiv/truvada/truvad.... Accessed 16 September 2020.
-
- Best BM, Burchett S, Li H, Stek A, Hu C, Wang J, Hawkins E, Byroads M, Watts DH, Smith E, Fletcher CV, Capparelli EV, Mirochnick M, International Maternal Pediatric and Adolescent AIDS Clinical Trials (IMPAACT) P1026s Team. 2015. Pharmacokinetics of tenofovir during pregnancy and postpartum. HIV Med 16:502–511. doi: 10.1111/hiv.12252. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- P30 AI094189/AI/NIAID NIH HHS/United States
- HHSN275201800001C/HD/NICHD NIH HHS/United States
- UL1 TR000124/TR/NCATS NIH HHS/United States
- UM1 AI068634/AI/NIAID NIH HHS/United States
- UM1 AI068616/AI/NIAID NIH HHS/United States
- K23 HD104517/HD/NICHD NIH HHS/United States
- UL1 TR000423/TR/NCATS NIH HHS/United States
- UL1 TR001881/TR/NCATS NIH HHS/United States
- UM1 AI106716/AI/NIAID NIH HHS/United States
- UL1 TR000154/TR/NCATS NIH HHS/United States
- UM1 AI068632/AI/NIAID NIH HHS/United States
- UM1 AI069536/AI/NIAID NIH HHS/United States
- HHSN275201800001I/HD/NICHD NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
