

Delayed atomoxetine or fluoxetine treatment coupled with limited voluntary running promotes motor recovery in mice after ischemic stroke
- PMID: 33318401
- PMCID: PMC8284259
- DOI: 10.4103/1673-5374.301031
Delayed atomoxetine or fluoxetine treatment coupled with limited voluntary running promotes motor recovery in mice after ischemic stroke
Abstract
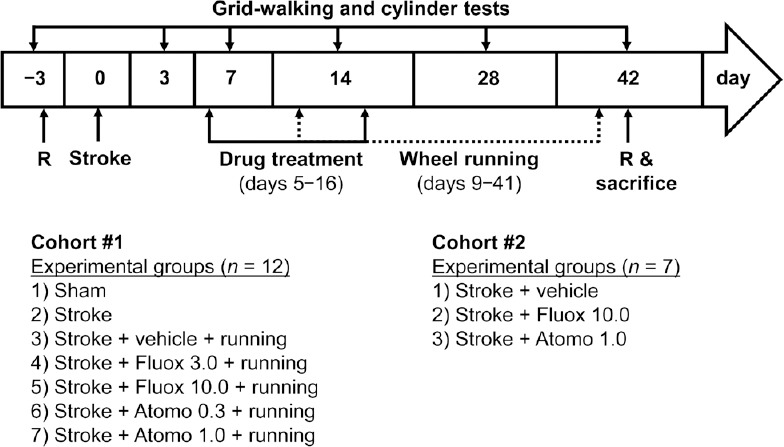
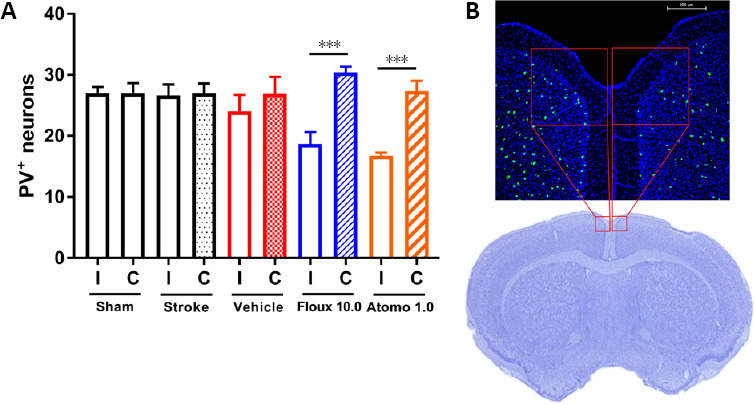
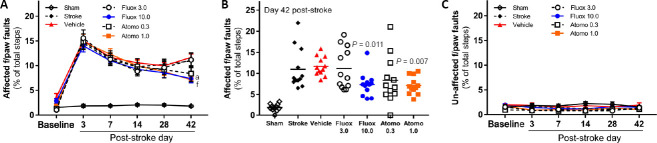
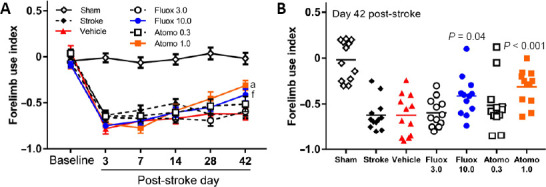
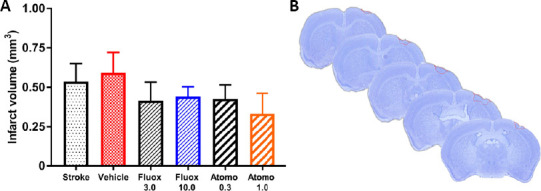
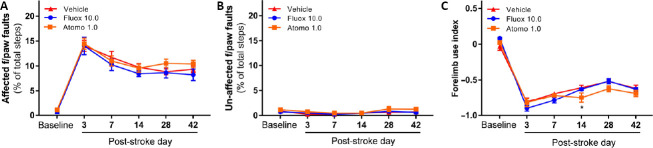
Currently, there is an unmet need for treatments promoting post-stroke functional recovery. The aim of this study was to evaluate and compare the dose-dependent effect of delayed atomoxetine or fluoxetine therapy (starting on post-stroke day 5), coupled with limited physical exercise (2 hours daily voluntary wheel running; post-stroke days 9 to 42), on motor recovery of adult male mice after photothrombotic stroke. These drugs are selective norepinephrine or serotonin reuptake inhibitors indicated for disorders unrelated to stroke. The predetermined primary end-point for this study was motor function measured in two tasks of spontaneous motor behaviors in grid-walking and cylinder tests. Additionally, we quantified the running distance and speed throughout the study, the number of parvalbumin-positive neurons in the medial agranular cortex and infarct volumes. Both sensorimotor tests revealed that neither limited physical exercise nor a drug treatment alone significantly facilitated motor recovery in mice after stroke. However, combination of physical exercise with either of the drugs promoted restoration of motor function by day 42 post-stroke, with atomoxetine being a more potent drug. This was accompanied by a significant decrease in parvalbumin-positive inhibitory interneurons in the ipsilateral medial agranular cortex of mice with recovering motor function, while infarct volumes were comparable among experimental groups. If further validated in larger studies, our observations suggest that add-on atomoxetine or fluoxetine therapy coupled with limited, structured physical rehabilitation could offer therapeutic modality for stroke survivors who have difficulty to engage in early, high-intensity physiotherapy. Furthermore, in light of the recently completed Assessment oF FluoxetINe In sTroke recoverY (AFFINITY) and Efficacy oF Fluoxetine-a randomisEd Controlled Trial in Stroke (EFFECTS) trials, our observations call for newly designed studies where fluoxetine or atomoxetine pharmacotherapy is evaluated in combination with structured physical rehabilitation rather than alone. This study was approved by the Texas Tech University Health Sciences Center Institutional Animal Care and Use Committee (protocol # 16019).
Keywords: FLAME trial; drug repurposing; neural repair; physical exercise; physiotherapy; post-stroke recovery; pre-clinical trial; selective norepinephrine reuptake inhibitor; selective serotonin reuptake inhibitor; stroke pharmacotherapy.
Conflict of interest statement
None
Figures

References
-
- Alamri FF, Shoyaib AA, Biggers A, Jayaraman S, Guindon J, Karamyan VT. Applicability of the grip strength and automated von Frey tactile sensitivity tests in the mouse photothrombotic model of stroke. Behav Brain Res. 2018;336:250–255. - PubMed
-
- Asadollahi M, Ramezani M, Khanmoradi Z, Karimialavijeh E. The efficacy comparison of citalopram, fluoxetine, and placebo on motor recovery after ischemic stroke: a double-blind placebo-controlled randomized controlled trial. Clin Rehabil. 2018;32:1069–1075. - PubMed
-
- Bernhardt J, Godecke E, Johnson L, Langhorne P. Early rehabilitation after stroke. Curr Opin Neurol. 2017a;30:48–54. - PubMed
-
- Bernhardt J, Hayward KS, Kwakkel G, Ward NS, Wolf SL, Borschmann K, Krakauer JW, Boyd LA, Carmichael ST, Corbett D, Cramer SC. Agreed definitions and a shared vision for new standards in stroke recovery research: The Stroke Recovery and Rehabilitation Roundtable taskforce. Int J Stroke. 2017b;12:444–450. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
