

Recovery from disorders of consciousness: mechanisms, prognosis and emerging therapies
- PMID: 33318675
- PMCID: PMC7734616
- DOI: 10.1038/s41582-020-00428-x
Recovery from disorders of consciousness: mechanisms, prognosis and emerging therapies
Abstract
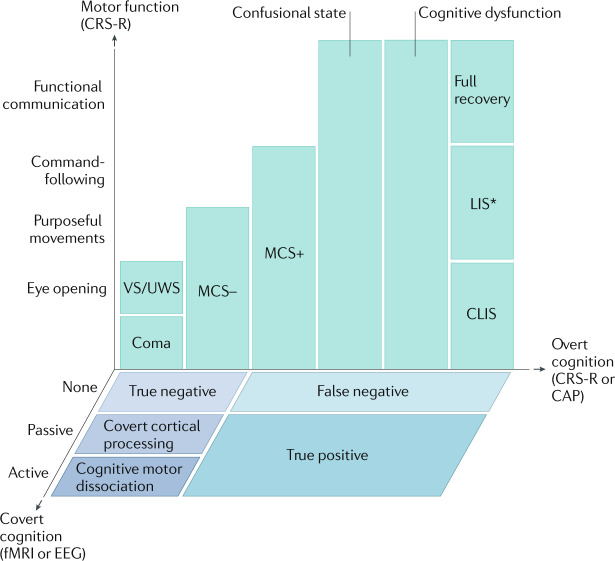
Substantial progress has been made over the past two decades in detecting, predicting and promoting recovery of consciousness in patients with disorders of consciousness (DoC) caused by severe brain injuries. Advanced neuroimaging and electrophysiological techniques have revealed new insights into the biological mechanisms underlying recovery of consciousness and have enabled the identification of preserved brain networks in patients who seem unresponsive, thus raising hope for more accurate diagnosis and prognosis. Emerging evidence suggests that covert consciousness, or cognitive motor dissociation (CMD), is present in up to 15-20% of patients with DoC and that detection of CMD in the intensive care unit can predict functional recovery at 1 year post injury. Although fundamental questions remain about which patients with DoC have the potential for recovery, novel pharmacological and electrophysiological therapies have shown the potential to reactivate injured neural networks and promote re-emergence of consciousness. In this Review, we focus on mechanisms of recovery from DoC in the acute and subacute-to-chronic stages, and we discuss recent progress in detecting and predicting recovery of consciousness. We also describe the developments in pharmacological and electrophysiological therapies that are creating new opportunities to improve the lives of patients with DoC.
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- Giacino JT, Fins JJ, Laureys S, Schiff ND. Disorders of consciousness after acquired brain injury: the state of the science. Nat. Rev. Neurol. 2014;10:99–114. - PubMed
-
- Giacino JT, et al. Practice guideline update recommendations summary: disorders of consciousness: report of the Guideline Development, Dissemination, and Implementation Subcommittee of the American Academy of Neurology; the American Congress of Rehabilitation Medicine; and the National Institute on Disability, Independent Living, and Rehabilitation Research. Neurology. 2018;91:450–460. - PMC - PubMed
-
- Teasdale G, Jennett B. Assessment of coma and impaired consciousness. A practical scale. Lancet. 1974;2:81–84. - PubMed
-
- Jennett B, Plum F. Persistent vegetative state after brain damage. A syndrome in search of a name. Lancet. 1972;1:734–737. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
