

Effects of dapagliflozin on prevention of major clinical events and recovery in patients with respiratory failure because of COVID-19: Design and rationale for the DARE-19 study
- PMID: 33319454
- PMCID: PMC8049025
- DOI: 10.1111/dom.14296
Effects of dapagliflozin on prevention of major clinical events and recovery in patients with respiratory failure because of COVID-19: Design and rationale for the DARE-19 study
Abstract
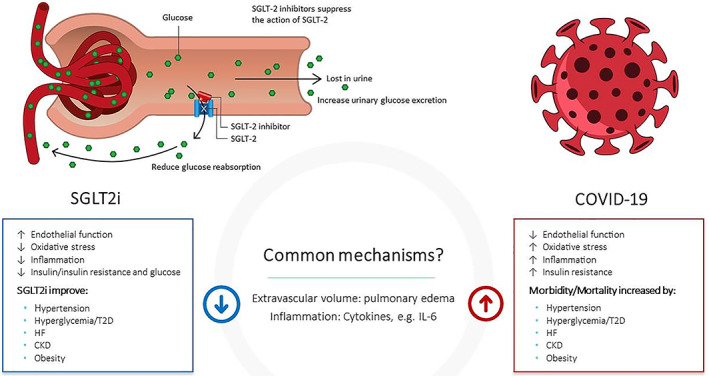
Aims: Coronavirus disease 2019 (COVID-19) is caused by a novel severe acute respiratory syndrome coronavirus 2. It can lead to multiorgan failure, including respiratory and cardiovascular decompensation, and kidney injury, with significant associated morbidity and mortality, particularly in patients with underlying metabolic, cardiovascular, respiratory or kidney disease. Dapagliflozin, a sodium-glucose cotransporter-2 inhibitor, has shown significant cardio- and renoprotective benefits in patients with type 2 diabetes (with and without atherosclerotic cardiovascular disease), heart failure and chronic kidney disease, and may provide similar organ protection in high-risk patients with COVID-19.
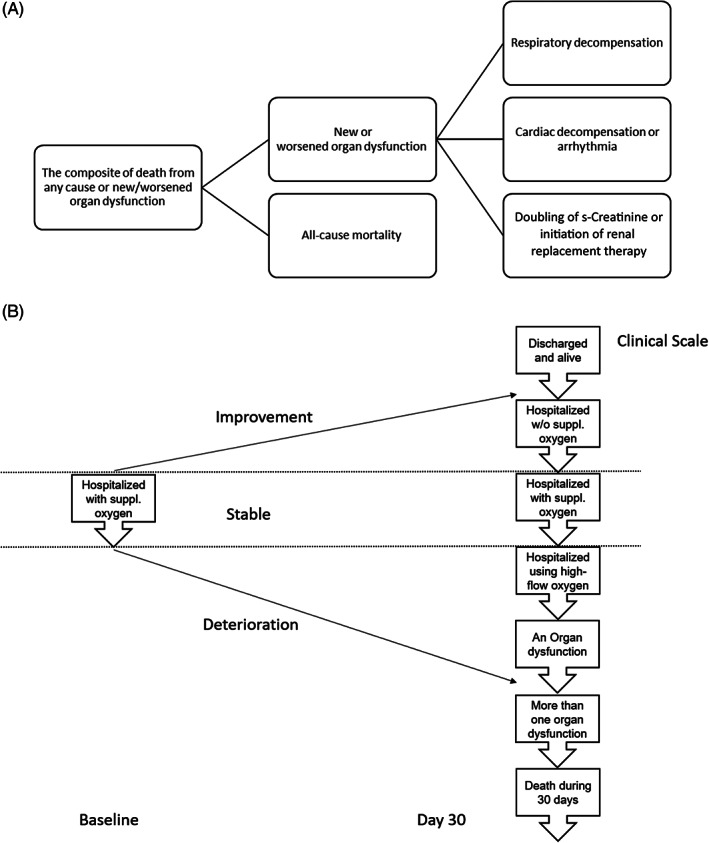
Materials and methods: DARE-19 (NCT04350593) is an investigator-initiated, collaborative, international, multicentre, randomized, double-blind, placebo-controlled study testing the dual hypotheses that dapagliflozin can reduce the incidence of cardiovascular, kidney and/or respiratory complications or all-cause mortality, or improve clinical recovery, in adult patients hospitalized with COVID-19 but not critically ill on admission. Eligible patients will have ≥1 cardiometabolic risk factor for COVID-19 complications. Patients will be randomized 1:1 to dapagliflozin 10 mg or placebo. Primary efficacy endpoints are time to development of new or worsened organ dysfunction during index hospitalization, or all-cause mortality, and the hierarchical composite endpoint of change in clinical status through day 30 of treatment. Safety of dapagliflozin in individuals with COVID-19 will be assessed.
Conclusions: DARE-19 will evaluate whether dapagliflozin can prevent COVID-19-related complications and all-cause mortality, or improve clinical recovery, and assess the safety profile of dapagliflozin in this patient population. Currently, DARE-19 is the first large randomized controlled trial investigating use of sodium-glucose cotransporter 2 inhibitors in patients with COVID-19.
Keywords: SGLT2 inhibitor; clinical trial; dapagliflozin; phase III study; randomized trial.
© 2020 The Authors. Diabetes, Obesity and Metabolism published by John Wiley & Sons Ltd.
Conflict of interest statement
M.K. has received a research grant for the conduct of this study from AstraZeneca. He has also received grant and research support from AstraZeneca outside the submitted work. He has received a grant and honoraria from Boehringer Ingelheim, and honoraria from Sanofi, Amgen, Novo Nordisk, Merck (Diabetes), Janssen, Bayer, Novartis, Applied Therapeutics, Amarin, Eli Lilly, and Vifor Pharma outside the submitted work. O.B. reports grants from AstraZeneca, Novartis, Bayer, Amgen, Boehringer‐Ingelheim and Pfizer, outside the submitted work. G.G.K. is the Principal Investigator of a biostatistics grant from AstraZeneca outside the submitted work. He is also the Principal Investigator for biostatistics grants from other biopharmaceutical sponsors that have no relationship to the submitted work. F.M. reports receiving honoraria from AstraZeneca for serving on the executive committee during the conduct of the study. O.M. has nothing to disclose. S.V. reports receiving grants, speaker honoraria and consulting fees from Boehringer‐Ingelheim, AstraZeneca, and Janssen during the conduct of this study. He has received speaker honoraria and consulting fees from Eli Lilly, and speaker honoraria from EOCI Pharmacomm Ltd, Sun Pharmaceuticals, and Toronto Knowledge Translation Working Group during the conduct of this study. He has also received grants and consulting fees from Amgen; grants, speaker honoraria and consulting fees from Bayer, and from Merck; grants from Bristol‐Myers Squibb; speaker honoraria and consulting fees from HLS Therapeutics, Novo Nordisk, and Sanofi; and speaker honoraria from Novartis outside the submitted work. V.C. declares no competing interests. A.J. received research support for this study from AstraZeneca. He has stock options in DexCom, and has a pending patent for fusion protein nanodiscs for the treatment of HF. P.A., S.B.G., J.B., C.D.S., A.M.L., J.O. and R.E. are employees and shareholders of AstraZeneca.
Figures

References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
