

Pulmonary Embolism and Deep Vein Thrombosis in COVID-19: A Systematic Review and Meta-Analysis
- PMID: 33320063
- PMCID: PMC7745997
- DOI: 10.1148/radiol.2020203557
Pulmonary Embolism and Deep Vein Thrombosis in COVID-19: A Systematic Review and Meta-Analysis
Abstract
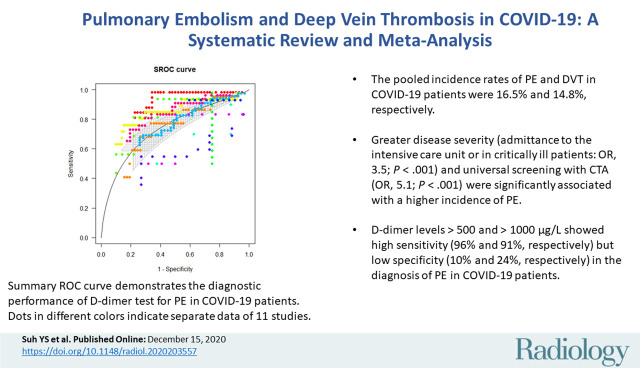
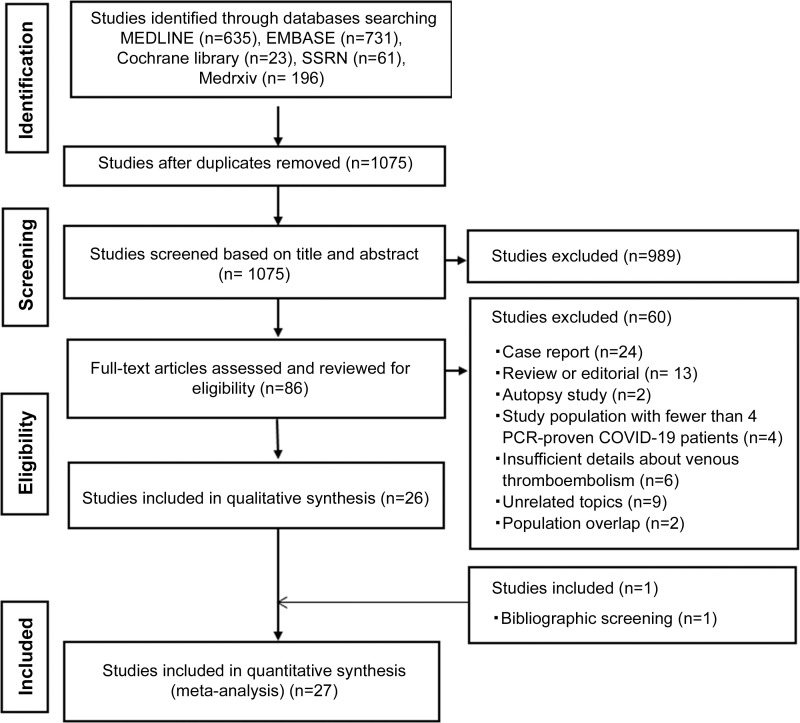
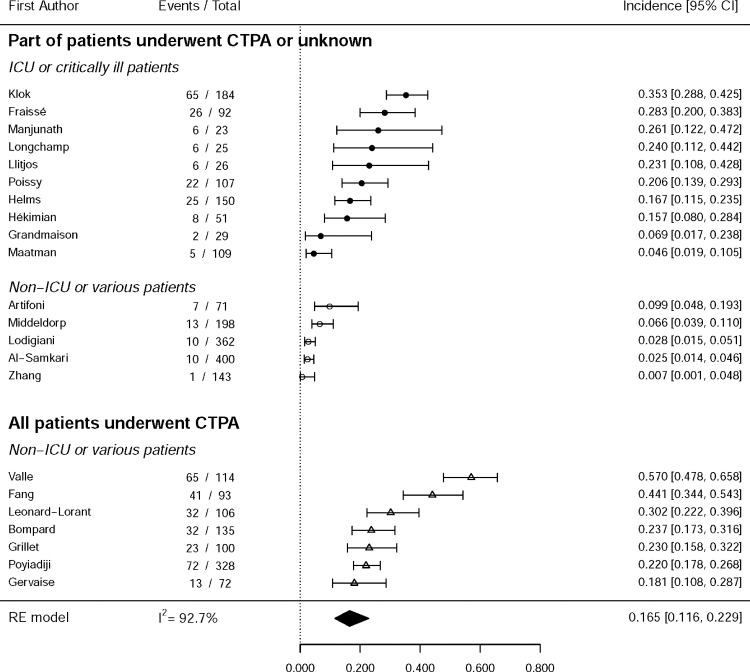
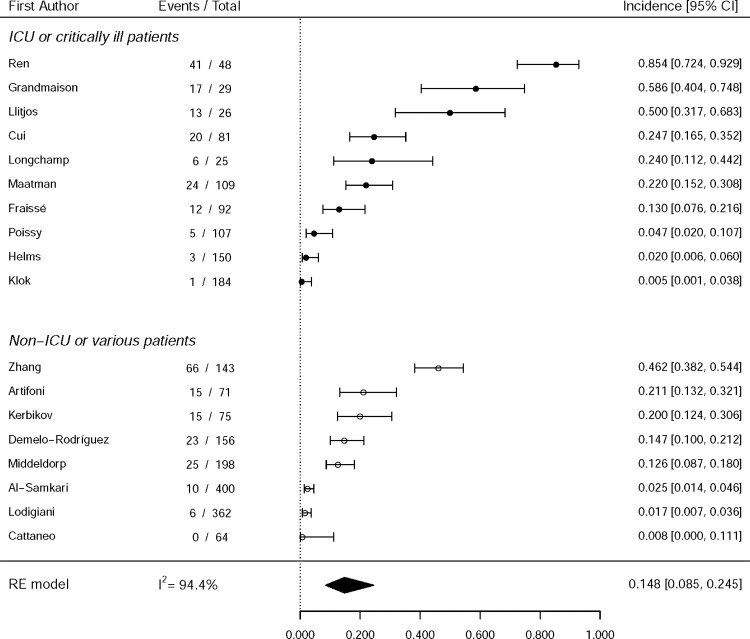
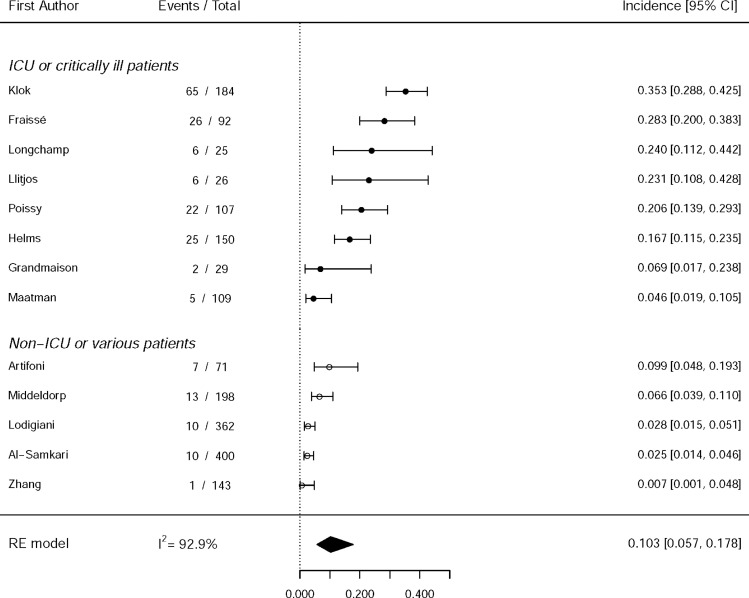
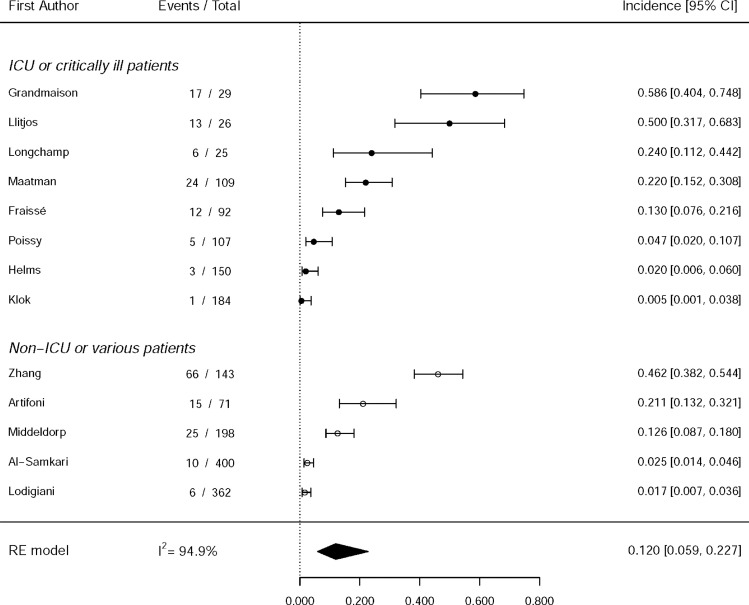
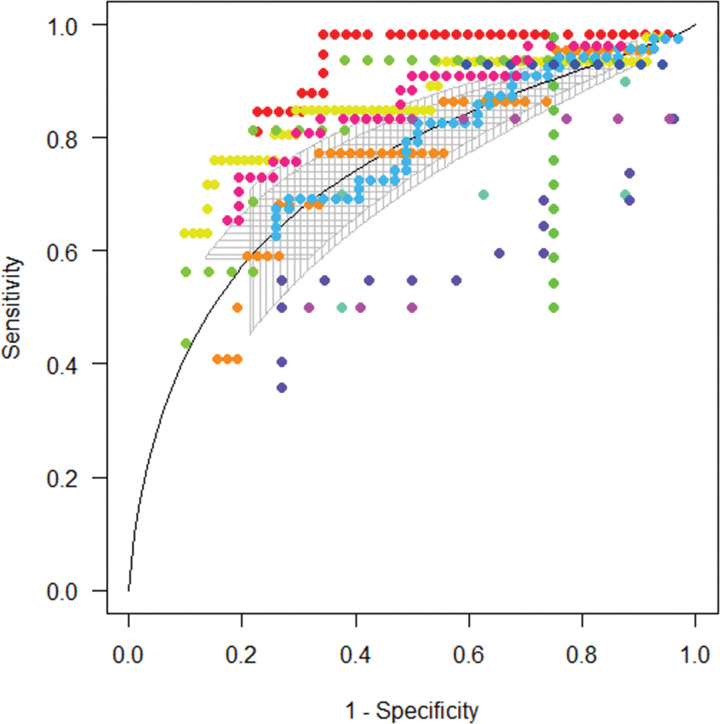
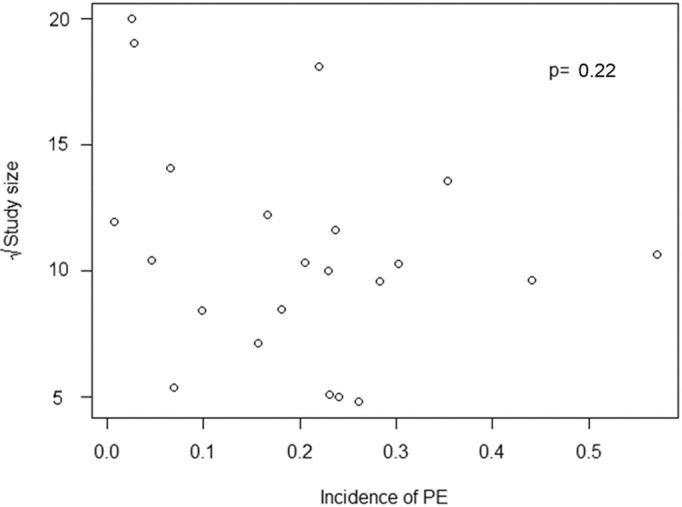
Background The association of pulmonary embolism (PE) with deep vein thrombosis (DVT) in patients with coronavirus disease 2019 (COVID-19) remains unclear, and the diagnostic accuracy of D-dimer tests for PE is unknown. Purpose To conduct meta-analysis of the study-level incidence of PE and DVT and to evaluate the diagnostic accuracy of D-dimer tests for PE from multicenter individual patient data. Materials and Methods A systematic literature search identified studies evaluating the incidence of PE or DVT in patients with COVID-19 from January 1, 2020, to June 15, 2020. These outcomes were pooled using a random-effects model and were further evaluated using metaregression analysis. The diagnostic accuracy of D-dimer tests for PE was estimated on the basis of individual patient data using the summary receiver operating characteristic curve. Results Twenty-seven studies with 3342 patients with COVID-19 were included in the analysis. The pooled incidence rates of PE and DVT were 16.5% (95% CI: 11.6, 22.9; I2 = 0.93) and 14.8% (95% CI: 8.5, 24.5; I2 = 0.94), respectively. PE was more frequently found in patients who were admitted to the intensive care unit (ICU) (24.7% [95% CI: 18.6, 32.1] vs 10.5% [95% CI: 5.1, 20.2] in those not admitted to the ICU) and in studies with universal screening using CT pulmonary angiography. DVT was present in 42.4% of patients with PE. D-dimer tests had an area under the receiver operating characteristic curve of 0.737 for PE, and D-dimer levels of 500 and 1000 μg/L showed high sensitivity (96% and 91%, respectively) but low specificity (10% and 24%, respectively). Conclusion Pulmonary embolism (PE) and deep vein thrombosis (DVT) occurred in 16.5% and 14.8% of patients with coronavirus disease 2019 (COVID-19), respectively, and more than half of patients with PE lacked DVT. The cutoffs of D-dimer levels used to exclude PE in preexisting guidelines seem applicable to patients with COVID-19. © RSNA, 2020 Supplemental material is available for this article. See also the editorial by Woodard in this issue.
Figures
Comment in
-
Pulmonary Thromboembolism in COVID-19.Radiology. 2021 Feb;298(2):E107-E108. doi: 10.1148/radiol.2020204175. Epub 2020 Dec 15. Radiology. 2021. PMID: 33325809 Free PMC article. No abstract available.
-
COVID-19 and Pulmonary Thromboembolism.Radiology. 2021 May;299(2):E252. doi: 10.1148/radiol.2021204709. Epub 2021 Mar 9. Radiology. 2021. PMID: 33687290 Free PMC article. No abstract available.
-
Pulmonary Embolism in COVID-19: The Actual Prevalence Remains Unclear.Radiology. 2021 May;299(2):E254. doi: 10.1148/radiol.2021204671. Epub 2021 Mar 16. Radiology. 2021. PMID: 33724068 Free PMC article. No abstract available.
-
CT Pulmonary Angiography for the Diagnosis of Pulmonary Embolism in Patients with COVID-19: When, Why, and for Who?Radiology. 2021 Jun;299(3):E287. doi: 10.1148/radiol.2021210400. Epub 2021 Mar 23. Radiology. 2021. PMID: 33754832 Free PMC article. No abstract available.
References
-
- World Health Organization . Coronavirus disease (COVID-19): situation report, 162. Geneva, Switzerland: World Health Organization, 2020.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
