

The Stanford Integrated Psychosocial Assessment for Transplant Is Associated With Outcomes Before and After Liver Transplantation
- PMID: 33320417
- PMCID: PMC9531321
- DOI: 10.1002/lt.25975
The Stanford Integrated Psychosocial Assessment for Transplant Is Associated With Outcomes Before and After Liver Transplantation
Abstract
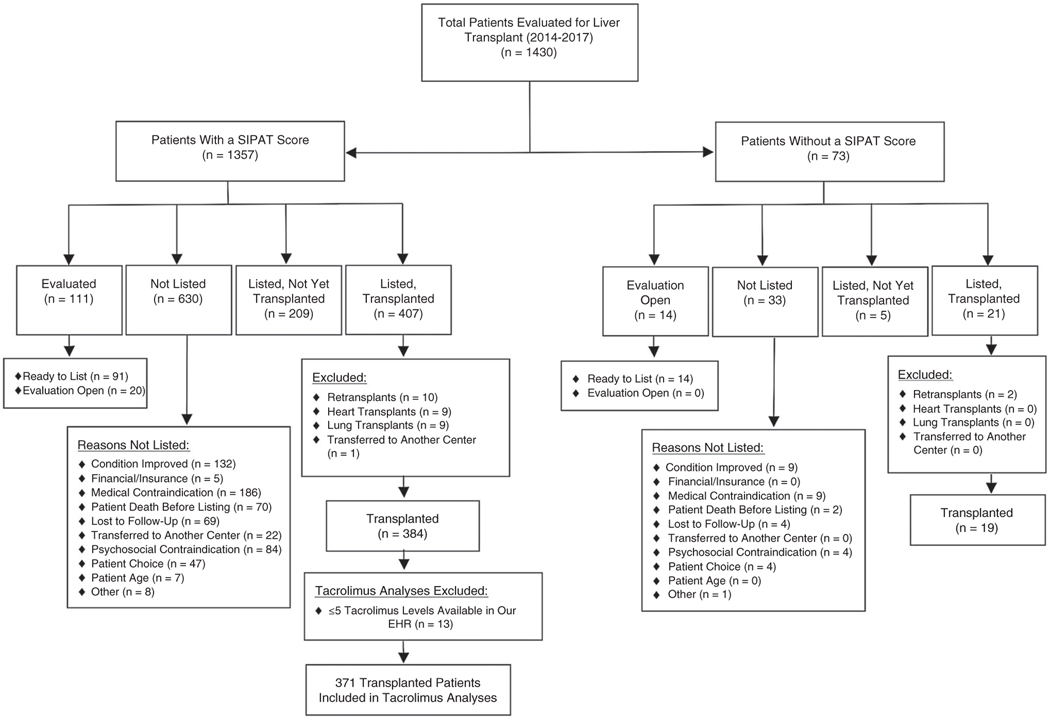
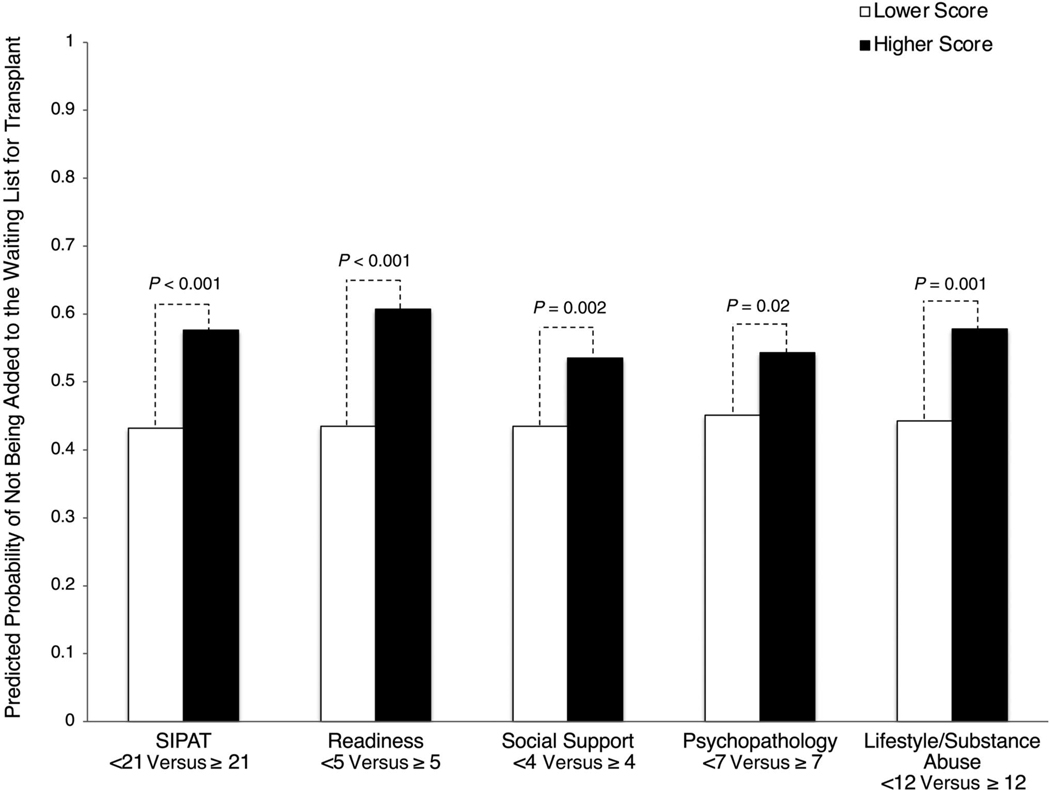
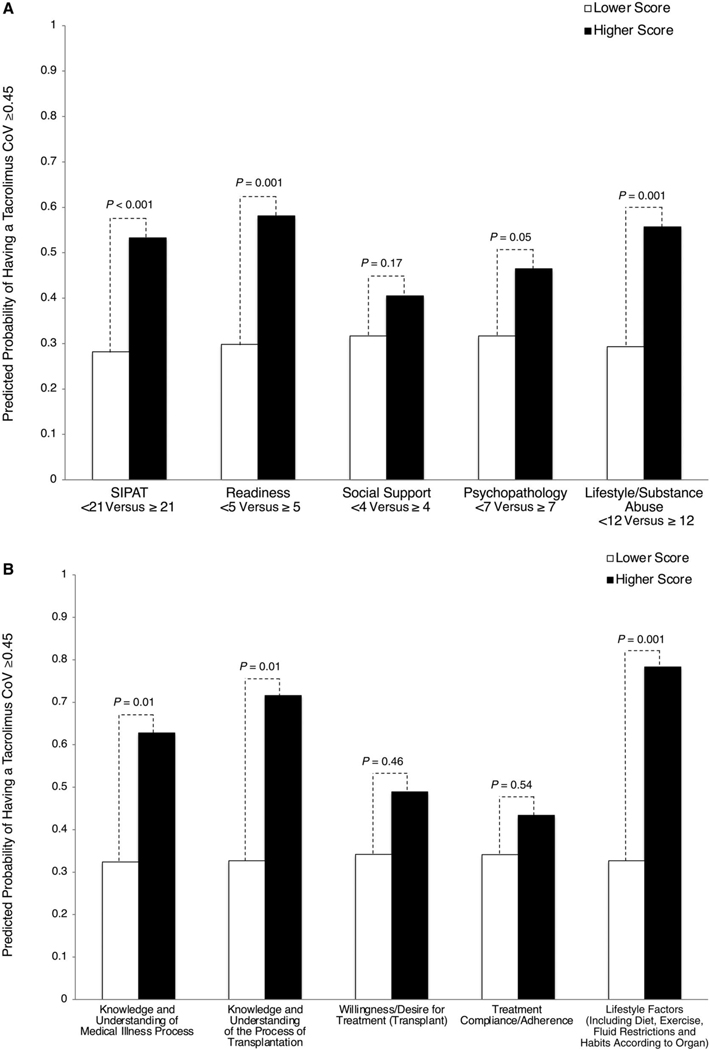
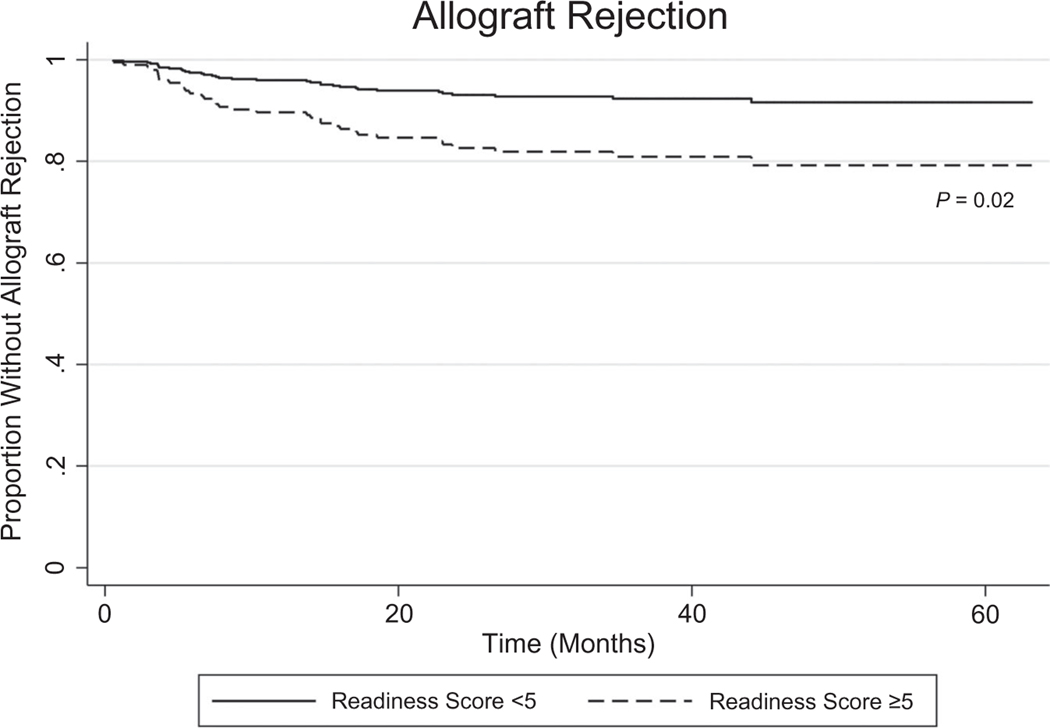
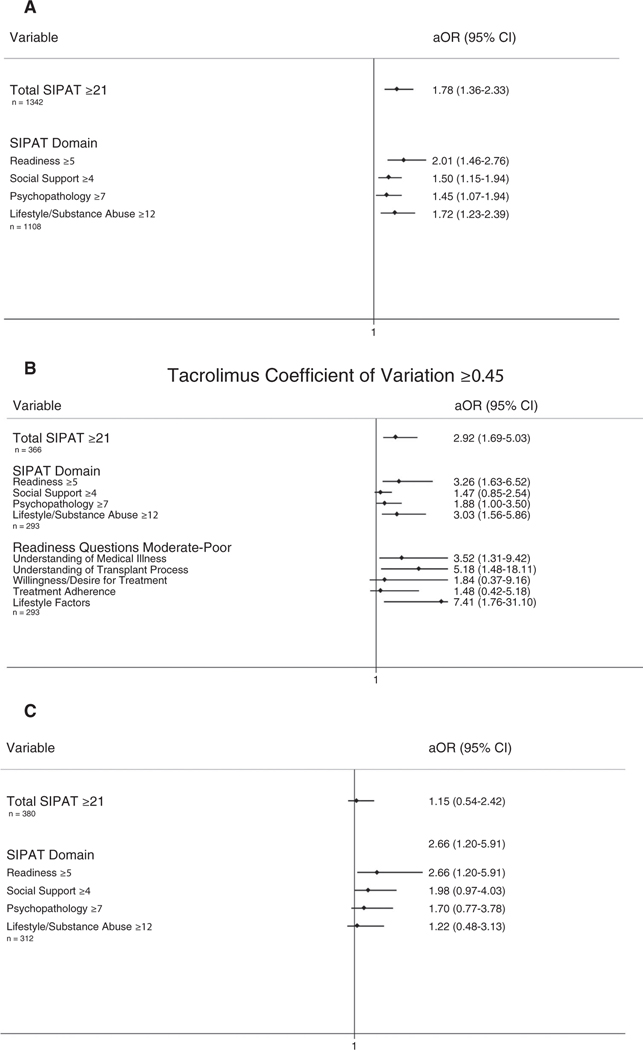
The Stanford Integrated Psychosocial Assessment for Transplant (SIPAT) is a standardized psychosocial evaluation tool used in liver transplantation (LT) evaluation. We assessed the impact of the SIPAT score and subdomains on transplant waitlisting decisions and post-LT outcomes including immunosuppression (IS) nonadherence, biopsy-proven rejection, andmortality/graft failure. We conducted a single-center observational cohort study of 1430 patients evaluated for LT. Patients were divided in 2 groups based on a SIPAT cutoff score of <21 or ≥21 (higher SIPAT scores indicate higher psychosocial risk). Regression models assessed relationships between total SIPAT score and domain scores and waitlisting decisions, IS nonadherence, allograft rejection, and death/graft failure. Elevated total SIPAT and SIPAT domain scores were associated not being added to the waitlist (total SIPAT core ≥21 adjusted odds ratio [aOR], 1.78 [95% confidence interval, CI, 1.36-2.33]; readiness score ≥5 aOR, 2.01 [95% CI, 1.36-2.76]; social support score ≥4aOR, 1.50 [95% CI, 1.15-1.94]; psychopathology score ≥7 aOR, 1.45 [95% CI, 1.07-1.94]; lifestyle/substance abuse score ≥12 aOR, 1.72 [95%CI, 1.23-2.39]) and were more likely to experience IS nonadherence as measured by the tacrolimus coefficient of variation (CoV) (total SIPAT score ≥21 aOR, 2.92 [95% CI, 1.69-5.03]; readiness score ≥5 aOR, 3.26 [95% CI, 1.63-6.52]; psychopathology score ≥7 aOR, 1.88 [95% CI, 1.00-3.50]; lifestyle substance abuse score ≥12 aOR, 3.03 [95% CI, 1.56-5.86]). SIPAT readinessscore ≥5 was associated with biopsy-proven allograft rejection (aOR, 2.66; 95% CI, 1.20-5.91). The SIPAT score was independently associated with LT listing decisions and IS nonadherence, and the readiness domain was associated with the risk of allograft rejection. These findings offer insights into higher risk recipients who require additional support before and aftertransplantation.
Copyright © 2020 by the American Association for the Study of Liver Diseases.
Figures
Comment in
-
Psychosocial Evaluation Matters.Liver Transpl. 2021 May;27(5):619-621. doi: 10.1002/lt.25992. Liver Transpl. 2021. PMID: 33484611 No abstract available.
-
Reply.Liver Transpl. 2021 Jun;27(6):938-939. doi: 10.1002/lt.25999. Liver Transpl. 2021. PMID: 33533537 Free PMC article. No abstract available.
-
Using Medication Level Variability to Predict Posttransplant Risk.Liver Transpl. 2021 Jun;27(6):936-937. doi: 10.1002/lt.26012. Liver Transpl. 2021. PMID: 33576115 No abstract available.
References
-
- Dew MA, Switzer GE, DiMartini AF, Matukaitis J, Fitzgerald MG, Kormos RL. Psychosocial assessments and outcomes in organ transplantation. Prog Transplant 2000;10:239–261. - PubMed
-
- Maldonado JR, Dubois HC, David EE, Sher Y, Lolak S, Dyal J, et al. The Stanford Integrated Psychosocial Assessment for Transplantation (SIPAT): a new tool for the psychosocial evaluation of pre-transplant candidates. Psychosomatics 2012;53:123–132. - PubMed
-
- Olbrisch ME, Levenson JL. Psychosocial assessment of organ transplant candidates. Current status of methodological and philosophical issues. Psychosomatics 1995;36:236–243. - PubMed
-
- Dobbels F, Verleden G, Dupont L, Vanhaecke J, De Geest S. To transplant or not? The importance of psychosocial and behavioural factors before lung transplantation. Chron Respir Dis 2006;3:39–47. - PubMed
-
- Dobbels F, De Geest S, Cleemput I, Fischler B, Kesteloot K, Vanhaecke J, et al. Psychosocial and behavioral selection criteria for solid organ transplantation. Prog Transplant 2001;11:121–132. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
