

Identification of Wee1 as a target in combination with avapritinib for gastrointestinal stromal tumor treatment
- PMID: 33320833
- PMCID: PMC7934848
- DOI: 10.1172/jci.insight.143474
Identification of Wee1 as a target in combination with avapritinib for gastrointestinal stromal tumor treatment
Abstract
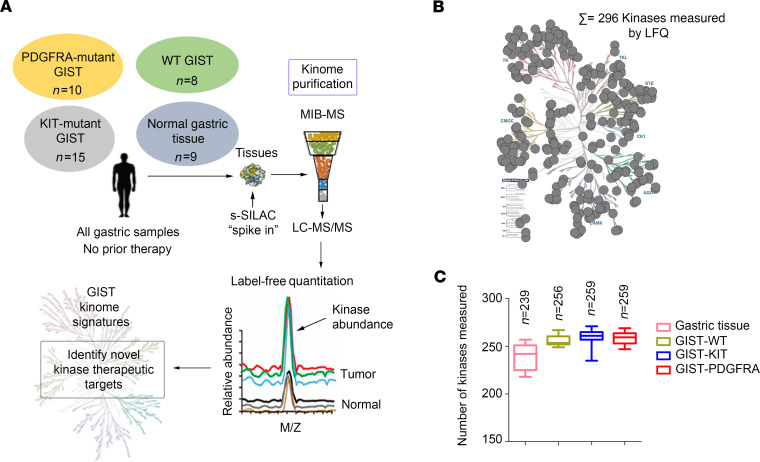
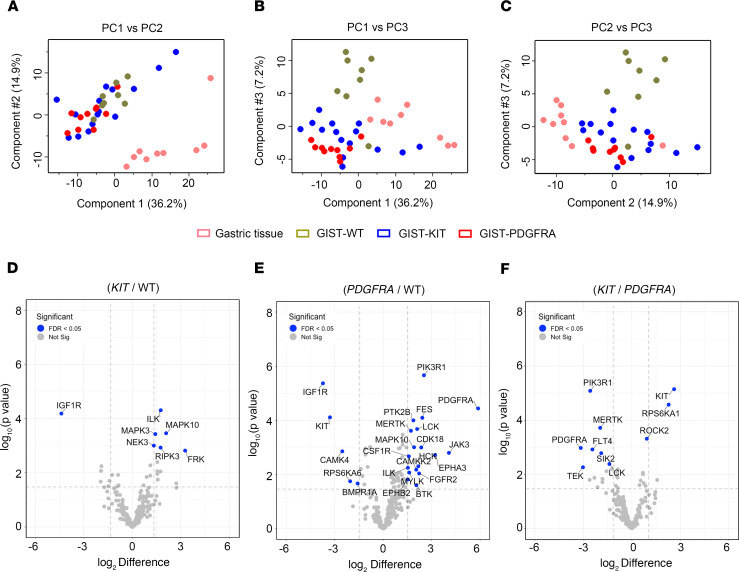
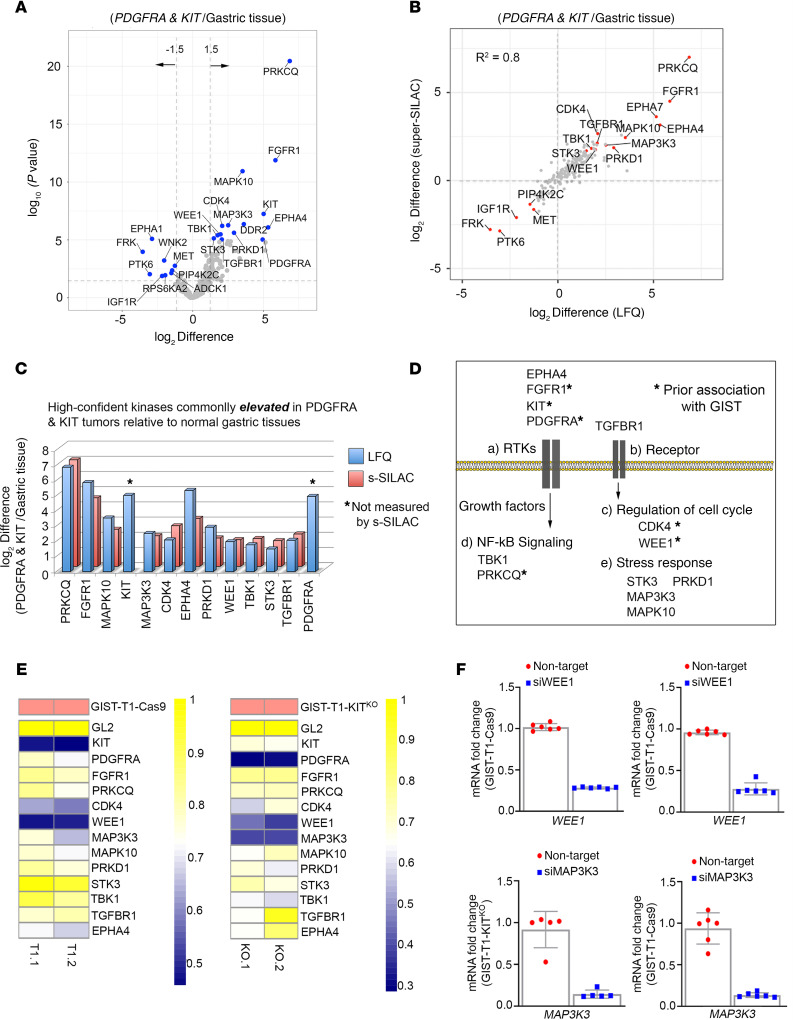
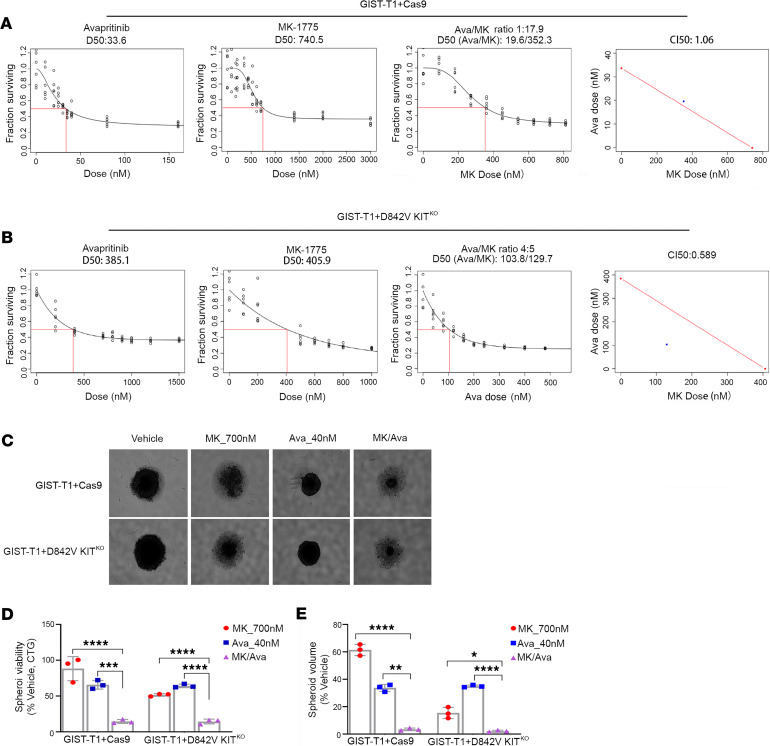
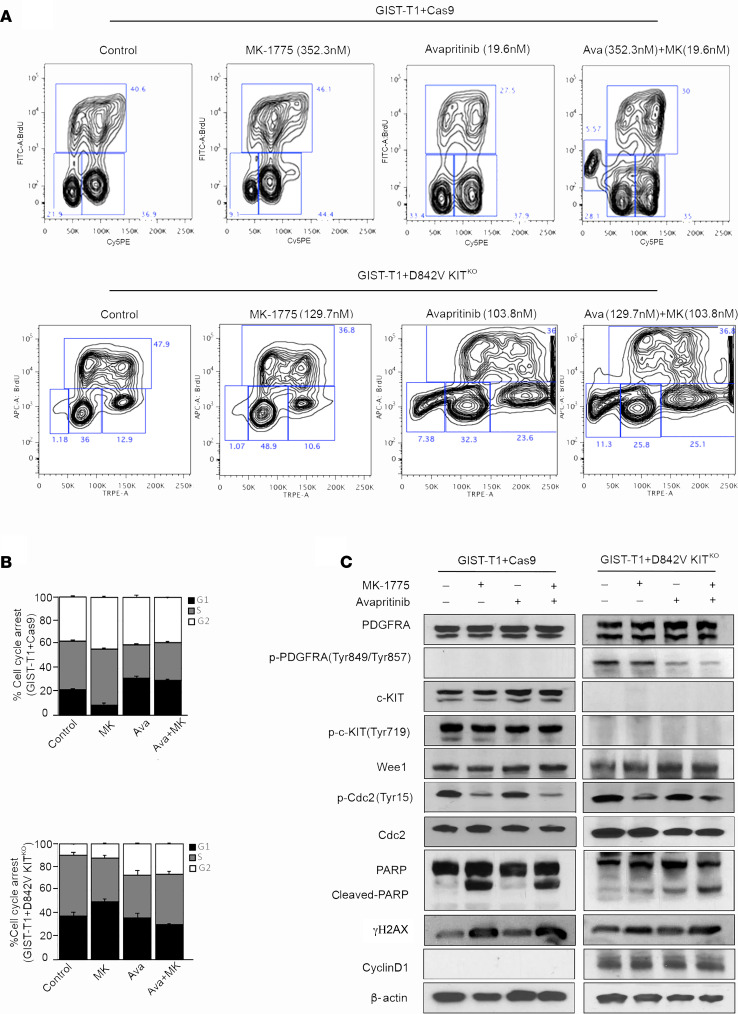
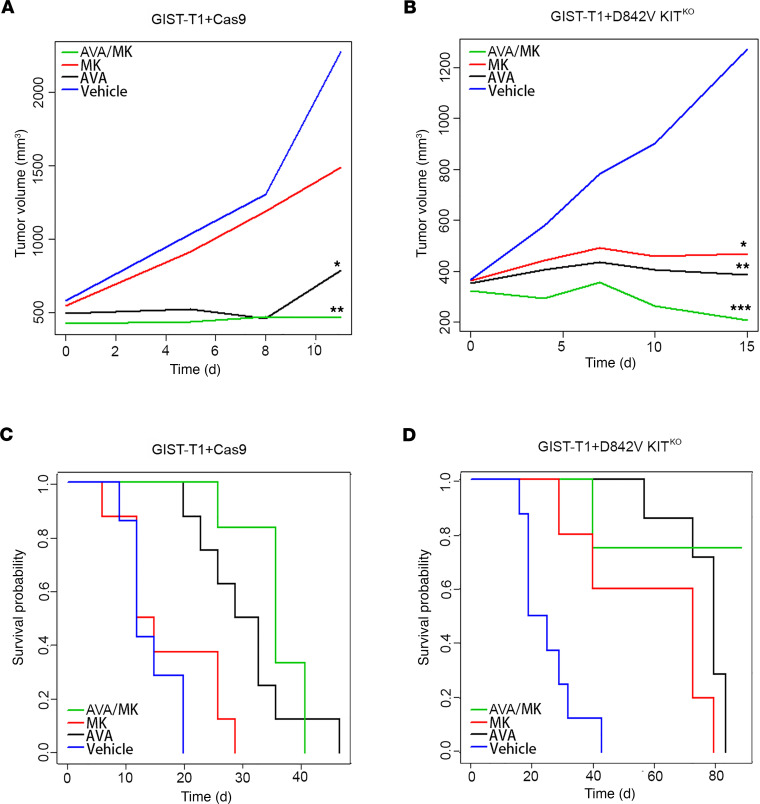
Management of gastrointestinal stromal tumors (GISTs) has been revolutionized by the identification of activating mutations in KIT and PDGFRA and clinical application of RTK inhibitors in advanced disease. Stratification of GISTs into molecularly defined subsets provides insight into clinical behavior and response to approved targeted therapies. Although these RTK inhibitors are effective in most GISTs, resistance remains a significant clinical problem. Development of effective treatment strategies for refractory GISTs requires identification of novel targets to provide additional therapeutic options. Global kinome profiling has the potential to identify critical signaling networks and reveal protein kinases essential in GISTs. Using multiplexed inhibitor beads and mass spectrometry, we explored the majority of the kinome in GIST specimens from the 3 most common molecular subtypes (KIT mutant, PDGFRA mutant, and succinate dehydrogenase deficient) to identify kinase targets. Kinome profiling with loss-of-function assays identified an important role for G2/M tyrosine kinase, Wee1, in GIST cell survival. In vitro and in vivo studies revealed significant efficacy of MK-1775 (Wee1 inhibitor) in combination with avapritinib in KIT mutant and PDGFRA mutant GIST cell lines as well as notable efficacy of MK-1775 as a monotherapy in the engineered PDGFRA mutant line. These studies provide strong preclinical justification for the use of MK-1775 in GIST.
Keywords: Cancer; Oncology; Therapeutics.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
