

PD-1 blockade improves Kupffer cell bacterial clearance in acute liver injury
- PMID: 33320839
- PMCID: PMC7880414
- DOI: 10.1172/JCI140196
PD-1 blockade improves Kupffer cell bacterial clearance in acute liver injury
Abstract
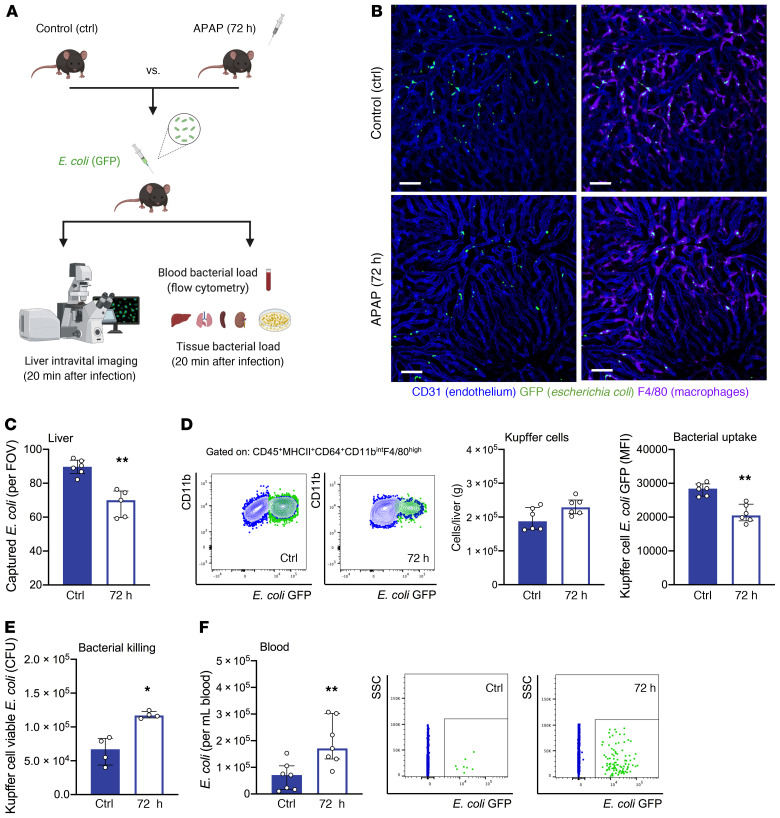
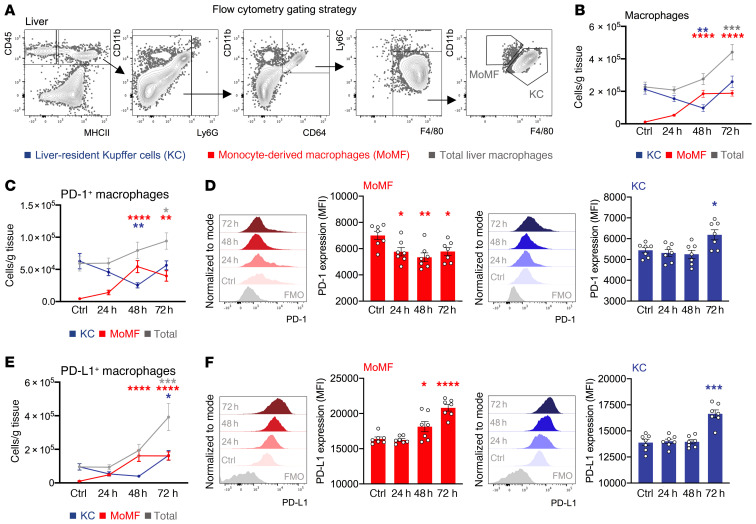
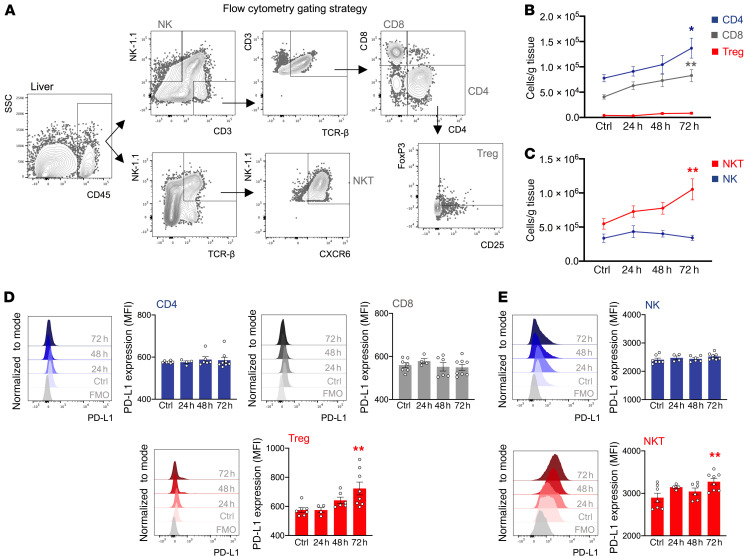
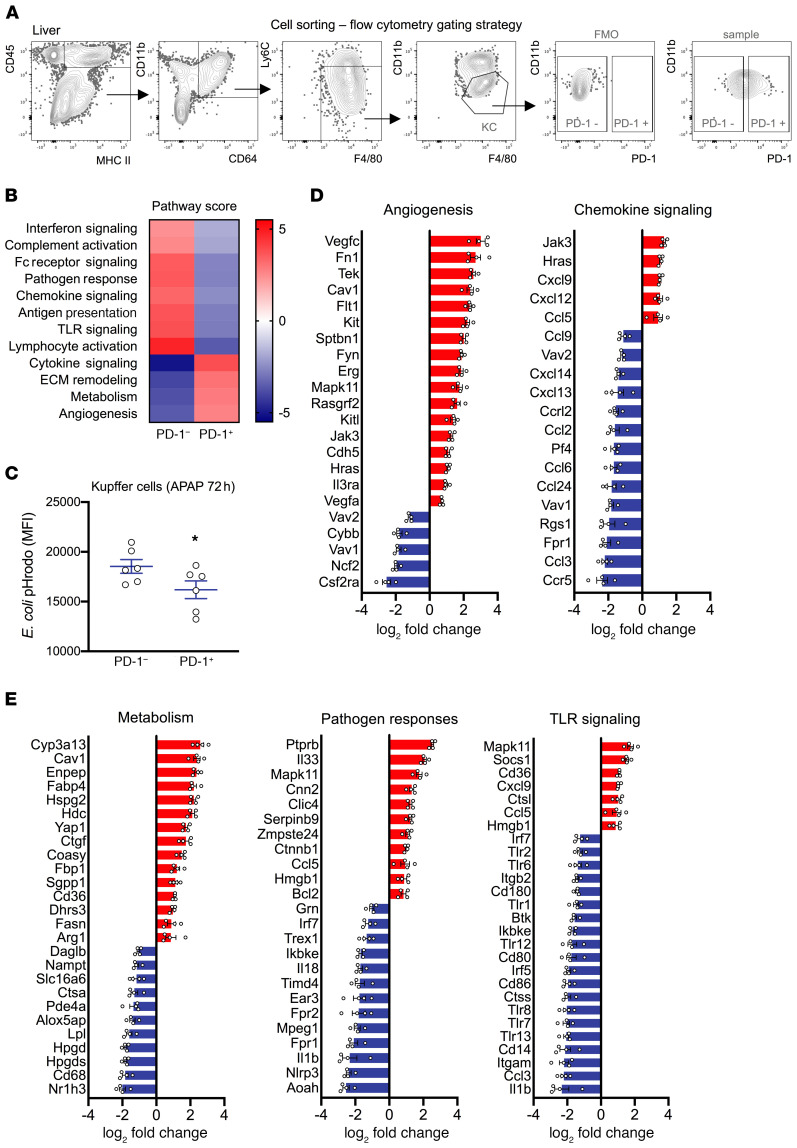
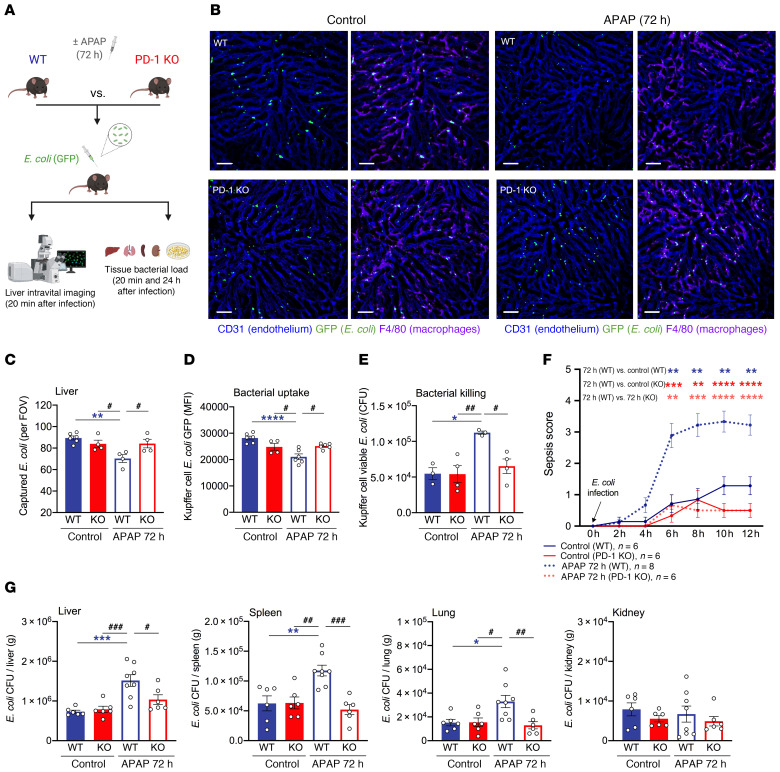
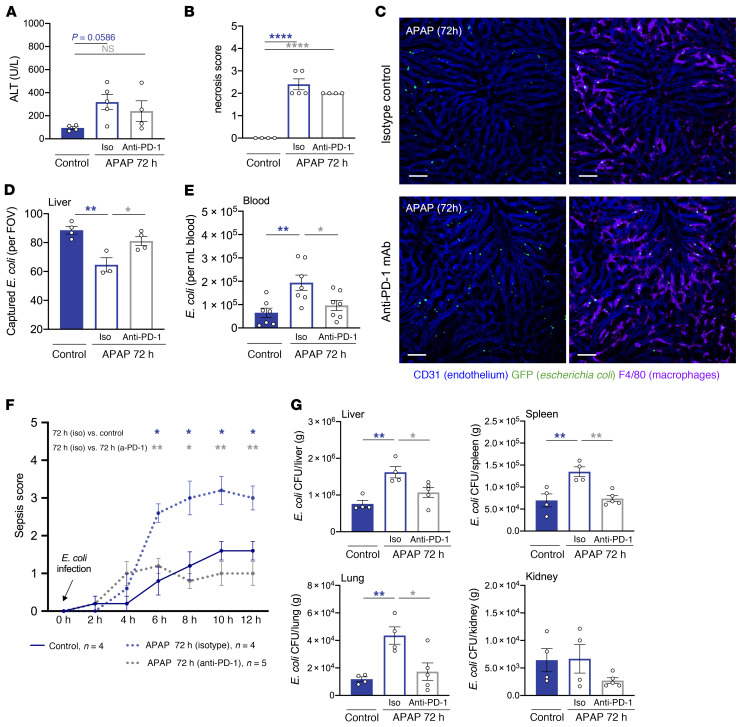
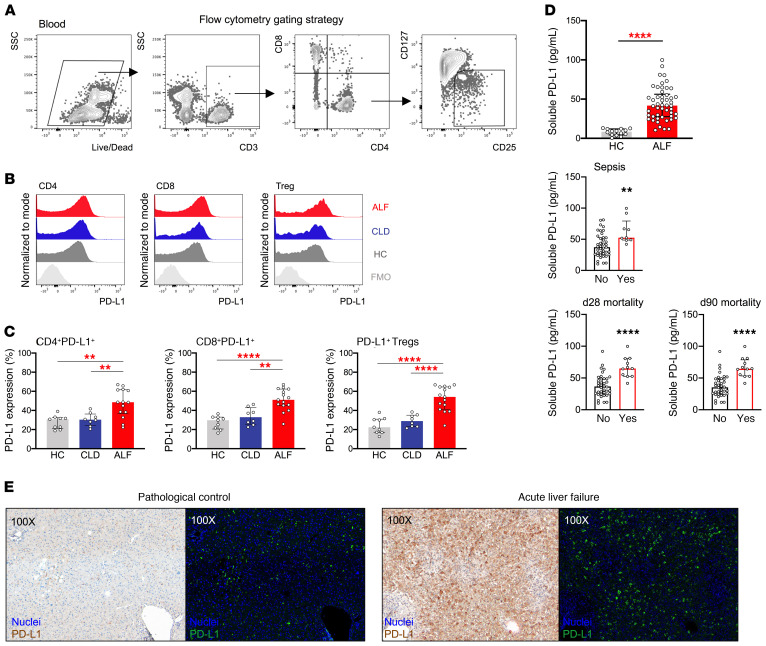
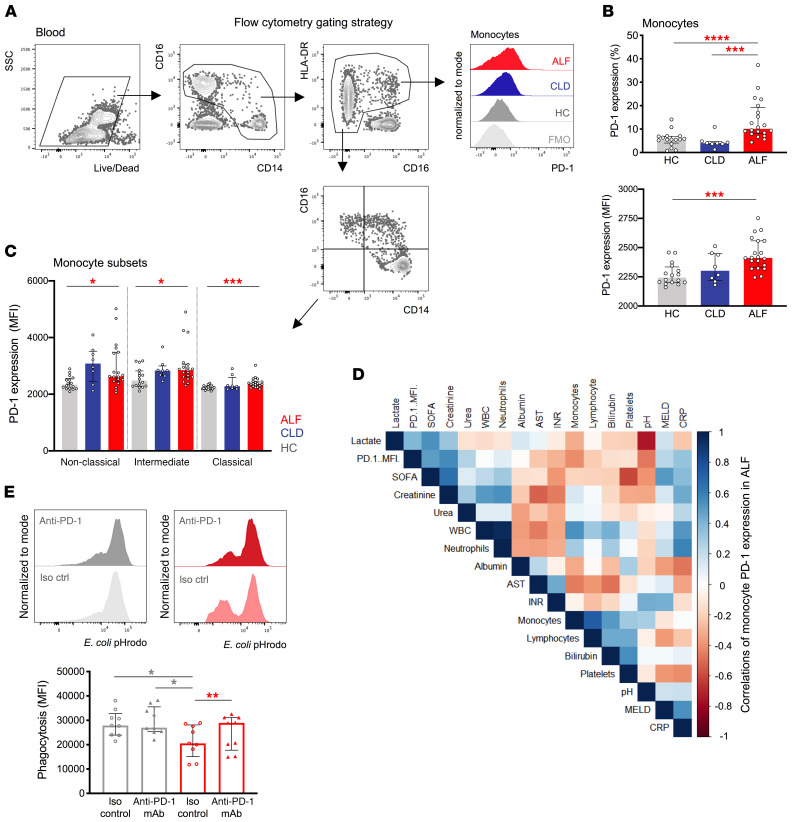
Patients with acute liver failure (ALF) have systemic innate immune suppression and increased susceptibility to infections. Programmed cell death 1 (PD-1) expression by macrophages has been associated with immune suppression during sepsis and cancer. We therefore examined the role of the programmed cell death 1/programmed death ligand 1 (PD-1/PD-L1) pathway in regulating Kupffer cell (KC) inflammatory and antimicrobial responses in acetaminophen-induced (APAP-induced) acute liver injury. Using intravital imaging and flow cytometry, we found impaired KC bacterial clearance and systemic bacterial dissemination in mice with liver injury. We detected increased PD-1 and PD-L1 expression in KCs and lymphocyte subsets, respectively, during injury resolution. Gene expression profiling of PD-1+ KCs revealed an immune-suppressive profile and reduced pathogen responses. Compared with WT mice, PD-1-deficient mice and anti-PD-1-treated mice with liver injury showed improved KC bacterial clearance, a reduced tissue bacterial load, and protection from sepsis. Blood samples from patients with ALF revealed enhanced PD-1 and PD-L1 expression by monocytes and lymphocytes, respectively, and that soluble PD-L1 plasma levels could predict outcomes and sepsis. PD-1 in vitro blockade restored monocyte functionality. Our study describes a role for the PD-1/PD-L1 axis in suppressing KC and monocyte antimicrobial responses after liver injury and identifies anti-PD-1 immunotherapy as a strategy to reduce infection susceptibility in ALF.
Keywords: Hepatology; Immunology; Innate immunity; Macrophages.
Conflict of interest statement
Figures
References
-
- Bernal W, et al. Acute liver failure: A curable disease by 2024? J Hepatol. 2015;62(S1):S112–S120. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
