

Congestive Hepatopathy
- PMID: 33321947
- PMCID: PMC7764741
- DOI: 10.3390/ijms21249420
Congestive Hepatopathy
Abstract
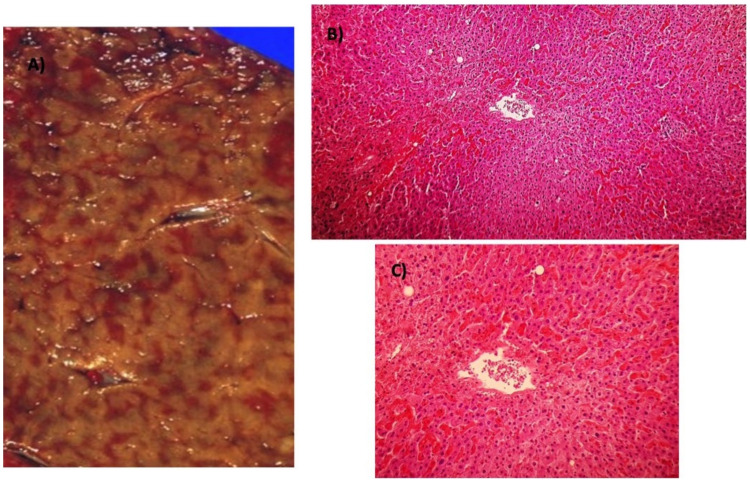
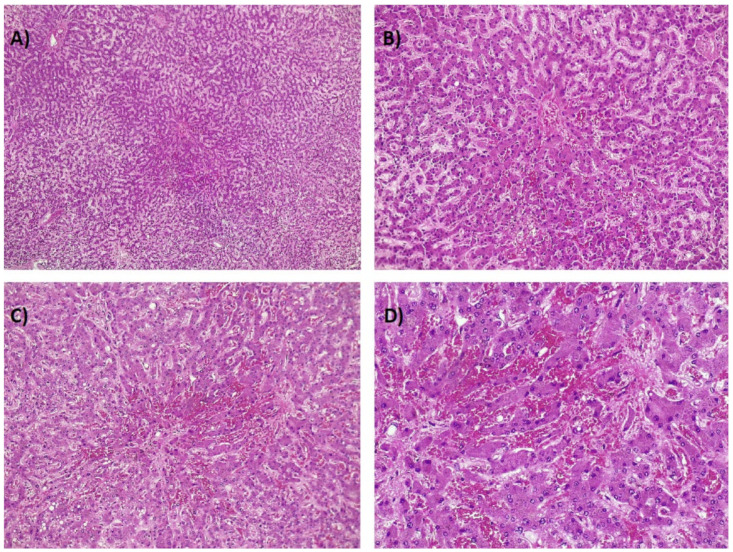
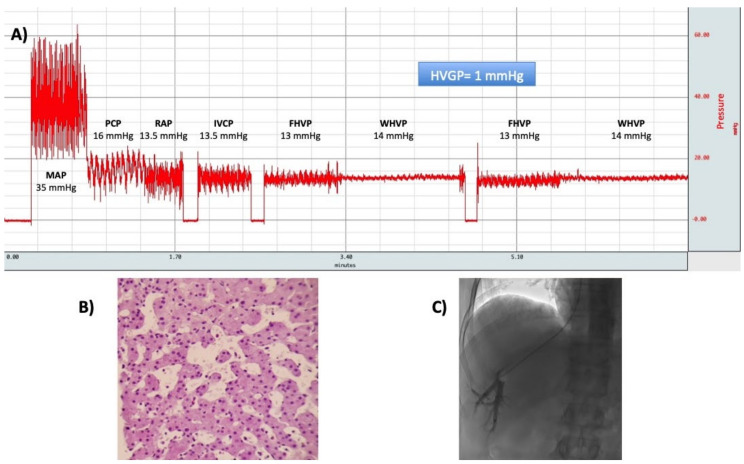
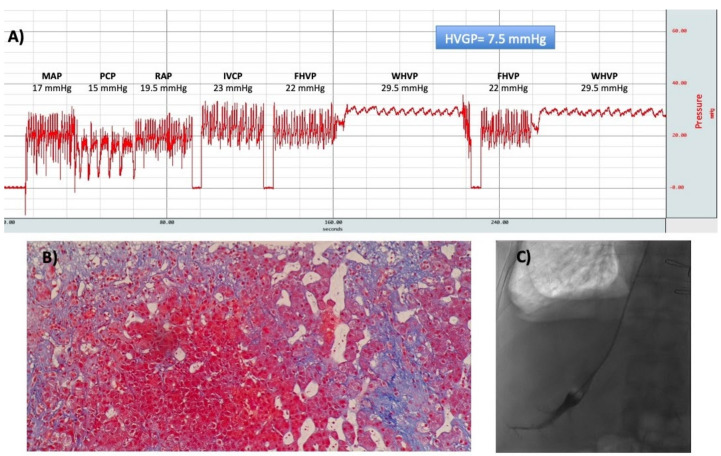
Liver disease resulting from heart failure (HF) has generally been referred as "cardiac hepatopathy". One of its main forms is congestive hepatopathy (CH), which results from passive venous congestion in the setting of chronic right-sided HF. The current spectrum of CH differs from earlier reports with HF, due to ischemic cardiomyopathy and congenital heart disease having surpassed rheumatic valvular disease. The chronic passive congestion leads to sinusoidal hypertension, centrilobular fibrosis, and ultimately, cirrhosis ("cardiac cirrhosis") and hepatocellular carcinoma after several decades of ongoing injury. Contrary to primary liver diseases, in CH, inflammation seems to play no role in the progression of liver fibrosis, bridging fibrosis occurs between central veins to produce a "reversed lobulation" pattern and the performance of non-invasive diagnostic tests of liver fibrosis is poor. Although the clinical picture and prognosis is usually dominated by the underlying heart condition, the improved long-term survival of cardiac patients due to advances in medical and surgical treatments are responsible for the increased number of liver complications in this setting. Eventually, liver disease could become as clinically relevant as cardiac disease and further complicate its management.
Keywords: cirrhosis; heart failure; heart transplantation; portal hypertension.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
