

CA125 and Ovarian Cancer: A Comprehensive Review
- PMID: 33322519
- PMCID: PMC7763876
- DOI: 10.3390/cancers12123730
CA125 and Ovarian Cancer: A Comprehensive Review
Abstract
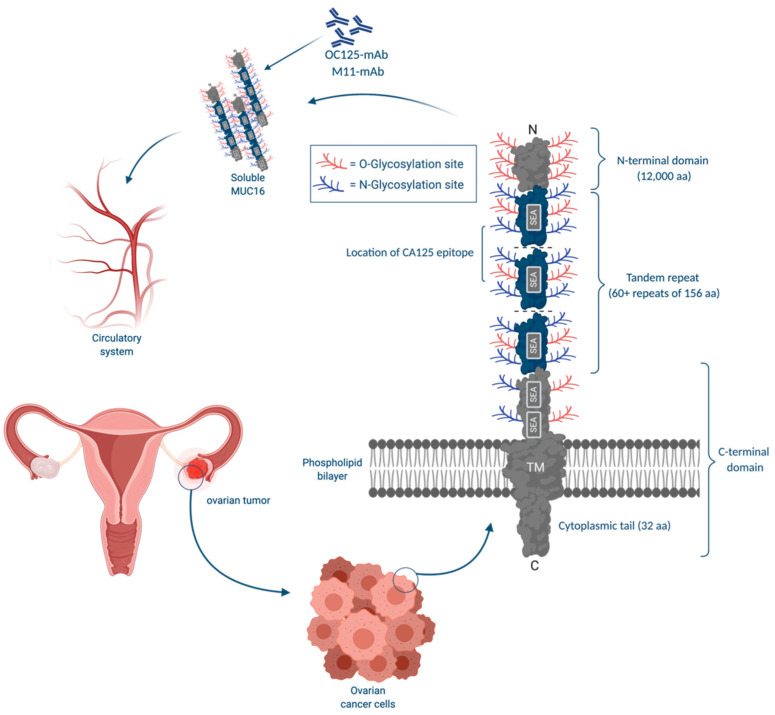
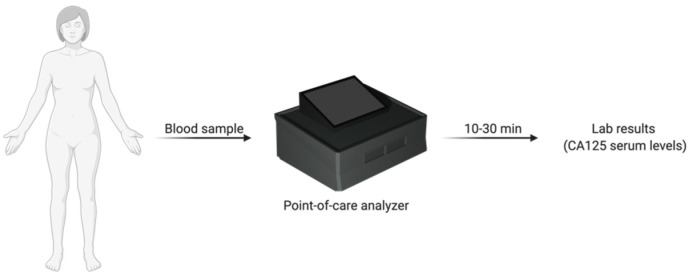
Ovarian cancer is the second most lethal gynecological malignancy. The tumour biomarker CA125 has been used as the primary ovarian cancer marker for the past four decades. The focus on diagnosing ovarian cancer in stages I and II using CA125 as a diagnostic biomarker has not improved patients' survival. Therefore, screening average-risk asymptomatic women with CA125 is not recommended by any professional society. The dualistic model of ovarian cancer carcinogenesis suggests that type II tumours are responsible for the majority of ovarian cancer mortality. However, type II tumours are rarely diagnosed in stages I and II. The recent shift of focus to the diagnosis of low volume type II ovarian cancer in its early stages of evolution provides a new and valuable target for screening. Type II ovarian cancers are usually diagnosed in advanced stages and have significantly higher CA125 levels than type I tumours. The detection of low volume type II carcinomas in stage IIIa/b is associated with a higher likelihood for optimal cytoreduction, the most robust prognostic indicator for ovarian cancer patients. The diagnosis of type II ovarian cancer in the early substages of stage III with CA125 may be possible using a higher cutoff point rather than the traditionally used 35 U/mL through the use of point-of-care CA125 assays in primary care facilities. Rapid point-of-care testing also has the potential for effective longitudinal screening and quick monitoring of ovarian cancer patients during and after treatment. This review covers the role of CA125 in the diagnosis and management of ovarian cancer and explores novel and more effective screening strategies with CA125.
Keywords: CA125; ovarian cancer; point-of-care; screening.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

References
-
- Howlader N., Noone A.M., Krapcho M., Miller D., Brest A., Yu M., Ruhl J., Tatalovich Z., Mariotto A., Lewis D.R., et al. SEER Cancer Statistics Review, 1975–2017. National Cancer Institute; Bethesda, MD, USA: 2020.
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
