

Safety and efficacy of intravenous thrombolysis in stroke patients on prior antiplatelet therapy in the WAKE-UP trial
- PMID: 33324940
- PMCID: PMC7678217
- DOI: 10.1186/s42466-020-00087-9
Safety and efficacy of intravenous thrombolysis in stroke patients on prior antiplatelet therapy in the WAKE-UP trial
Abstract
Background: One quarter to one third of patients eligible for systemic thrombolysis are on antiplatelet therapy at presentation. In this study, we aimed to assess the safety and efficacy of intravenous thrombolysis in stroke patients on prescribed antiplatelet therapy in the WAKE-UP trial.
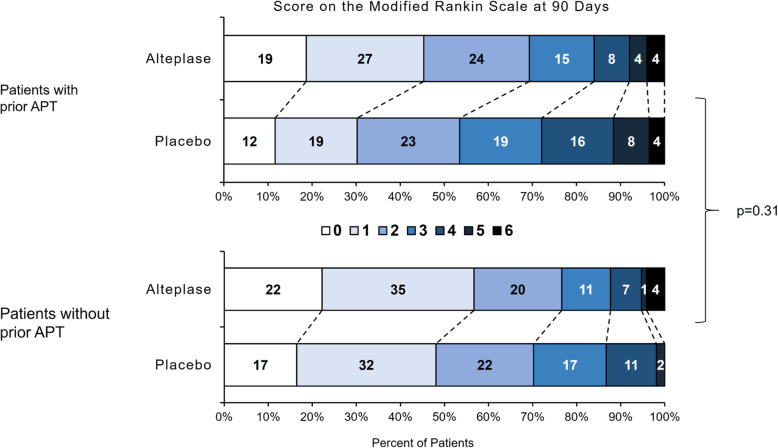
Methods: WAKE-UP was a multicenter, randomized, double-blind, placebo-controlled clinical trial to study the efficacy and safety of MRI-guided intravenous thrombolysis with alteplase in patients with an acute stroke of unknown onset time. The medication history of all patients randomized in the WAKE-UP trial was documented. The primary safety outcome was any sign of hemorrhagic transformation on follow-up MRI. The primary efficacy outcome was favorable functional outcome defined by a score of 0-1 on the modified Rankin scale at 90 days after stroke, adjusted for age and baseline stroke severity. Logistic regression models were fitted to study the association of prior antiplatelet treatment with outcome and treatment effect of intravenous alteplase.
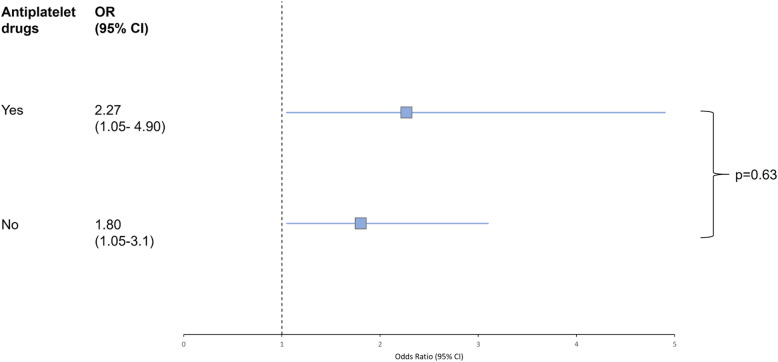
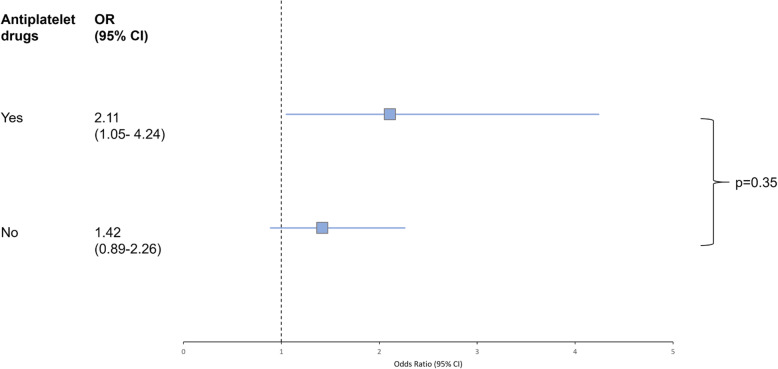
Results: Of 503 randomized patients, 164 (32.6%) were on antiplatelet treatment. Patients on antiplatelet treatment were older (70.3 vs. 62.8 years, p < 0.001), and more frequently had a history of hypertension, atrial fibrillation, diabetes, hypercholesterolemia, and previous stroke or transient ischaemic attack. Rates of symptomatic intracranial hemorrhage and hemorrhagic transformation on follow-up imaging did not differ between patients with and without antiplatelet treatment. Patients on prior antiplatelet treatment were less likely to achieve a favorable outcome (37.3% vs. 52.6%, p = 0.014), but there was no interaction of prior antiplatelet treatment with intravenous alteplase concerning favorable outcome (p = 0.355). Intravenous alteplase was associated with higher rates of favorable outcome in patients on prior antiplatelet treatment with an adjusted odds ratio of 2.106 (95% CI 1.047-4.236).
Conclusions: Treatment benefit of intravenous alteplase and rates of post-treatment hemorrhagic transformation were not modified by prior antiplatelet intake among MRI-selected patients with unknown onset stroke. Worse functional outcome in patients on antiplatelets may result from a higher load of cardiovascular co-morbidities in these patients.
Keywords: Alteplase; Antiplatelet; Aspirin; Clopidogrel; Hemorrhagic transformation; Ischemic stroke; Recombinant human tissue plasminogen activator; Rt-PA; Thrombolysis; WAKE UP.
© The Author(s) 2020.
Conflict of interest statement
Competing interestsEB reports grants from the German Parkinson Society and ACTELION Pharmaceuticals Deutschland GmbH, outside the submitted work. FB reports grants from University Medical Center Hamburg-Eppendorf during the conduct of the study. ME reports grants from Bayer and fees paid to the Charité from Bayer, Boehringer Ingelheim, BMS/Pfizer, Daiichi Sankyo, Amgen, GlaxoSmithKlineGSK, Sanofi, Covidien, Ever, Novartis, all outside the submitted work. JBF reports personal fees from Bioclinica, Artemida, Cerevast, and Nicolab outside the submitted work. TM reports grants from DFG, BMBF, the Schilling Foundation, Merck-Serono and Grifols, outside the submitted work. VT reports personal fees and non-financial support from Boehringer Ingelheim, Pfizer/BMS, Bayer, Sygnis, Amgen and Allergan outside the submitted work. KWM reports personal fees and non-financial support from Boehringer Ingelheim outside the submitted work. CZS reports grants from Novo Nordisk Foundation and personal fees from Bayer outside the submitted work. CG reports personal. fees from AMGEN, Bayer Vital, BMS, Boehringer Ingelheim, Sanofi Aventis, Abbott, and Prediction Biosciences outside the submitted work. GT reports personal fees from Acandis, Boehringer Ingelheim, BMS/Pfizer, Stryker, Portola, Daiichi Sankyo, grants and personal fees from Bayer, grants from Corona Foundation, German Innovation Fonds and Else Kroener Fresenius Foundation outside the submitted work. All remaining authors declare no competing interests.
Figures
References
-
- Dowlatshahi D, Hakim A, Fang J, Sharma M, Investigators of the Registry of the Canadian Stroke Network Pre admission antithrombotics are associated with improved outcomes following ischaemic stroke: a cohort from the registry of the Canadian stroke network. International Journal of Stroke : Official Journal of the International Stroke Society. 2009;4(5):328–334. doi: 10.1111/j.1747-4949.2009.00331.x. - DOI - PubMed
-
- Malhotra K, Katsanos AH, Goyal N, Ahmed N, Strbian D, Palaiodimou L, et al. Safety and efficacy of dual antiplatelet pretreatment in patients with ischemic stroke treated with IV thrombolysis: a systematic review and meta-analysis. Neurology. 2020;94(7):e657–e666. doi: 10.1212/WNL.0000000000008961. - DOI - PubMed
LinkOut - more resources
Full Text Sources