

Performance evaluation of antibody tests for detecting infant respiratory syncytial virus infection
- PMID: 33325064
- PMCID: PMC8046717
- DOI: 10.1002/jmv.26736
Performance evaluation of antibody tests for detecting infant respiratory syncytial virus infection
Abstract
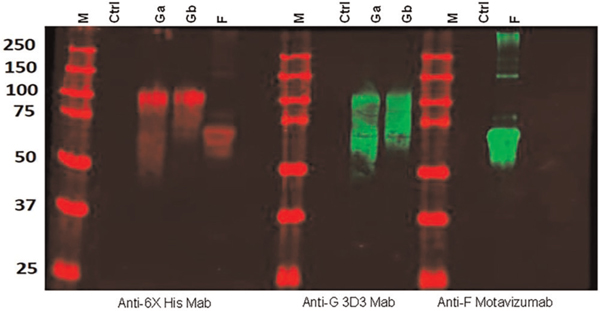
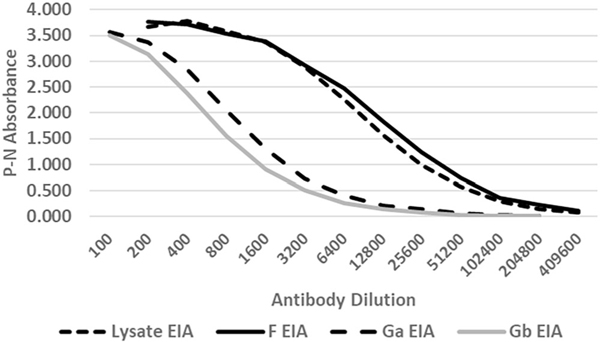
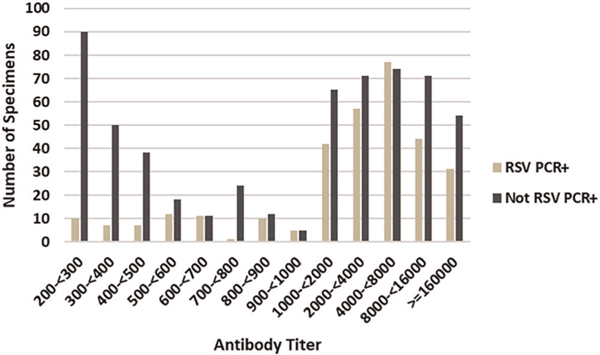
Respiratory syncytial virus (RSV) infection is a major cause of respiratory tract disease in young children and throughout life. Infant infection is also associated with later respiratory morbidity including asthma. With a prospective birth cohort study of RSV and asthma, we evaluated the performance of an RSV antibody enzyme-linked immunoassay (EIA) for detecting prior infant RSV infection. Infant RSV infection was determined by biweekly respiratory illness surveillance plus RSV polymerase chain reaction (PCR) testing in their first RSV season and serum RSV antibodies after the season at approximately 1 year of age. RSV antibodies were detected by RSV A and B lysate EIA. Antibody and PCR results on 1707 children included 327 RSV PCR positive (PCR+) and 1380 not RSV+. Of 327 PCR+ children, 314 (96%) were lysate EIA positive and 583 out of 1380 (42%) children not PCR+ were positive. We compared the lysate EIA to RSV F, group A G (Ga), and group B G (Gb) protein antibody EIAs in a subset of 226 sera, 118 PCR+ children (97 group A and 21 group B) and 108 not PCR+. In this subset, 117 out of 118 (99%) RSV PCR+ children were positive by both the F and lysate EIAs and 103 out of 118 (87%) were positive by the Ga and/or Gb EIAs. Comparison of the two G EIAs indicated the infecting group correctly in 100 out of 118 (86%) and incorrectly in 1 out of 118 (1%). The lysate and F EIAs are sensitive for detecting infant infection and the two G EIAs can indicate the group of an earlier primary infection.
Keywords: antibodies; infant; infection; respiratory syncytial virus.
© 2020 Wiley Periodicals LLC.
Conflict of interest statement
CONFLICT OF INTERESTS
The authors do not have conflicts related to the contents of this manuscript.
Figures
References
-
- Stockman LJ, Curns AT, Anderson LJ, Fischer-Langley G. Respiratory syncytial virus-associated hospitalizations among infants and young children in the United States, 1997–2006. Pediatr Infect Dis J. 2012; 31(1):5–9. - PubMed
-
- Ebihara T, Endo R, Kikuta H, Ishiguro N, Ishiko H, Kobayashi K. Comparison of the seroprevalence of human metapneumovirus and human respiratory syncytial virus. J Med Virol. 2004;72(2):304–306. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
