

Characterizing Pharmacogenetic Testing Among Children's Hospitals
- PMID: 33325650
- PMCID: PMC7993279
- DOI: 10.1111/cts.12931
Characterizing Pharmacogenetic Testing Among Children's Hospitals
Abstract
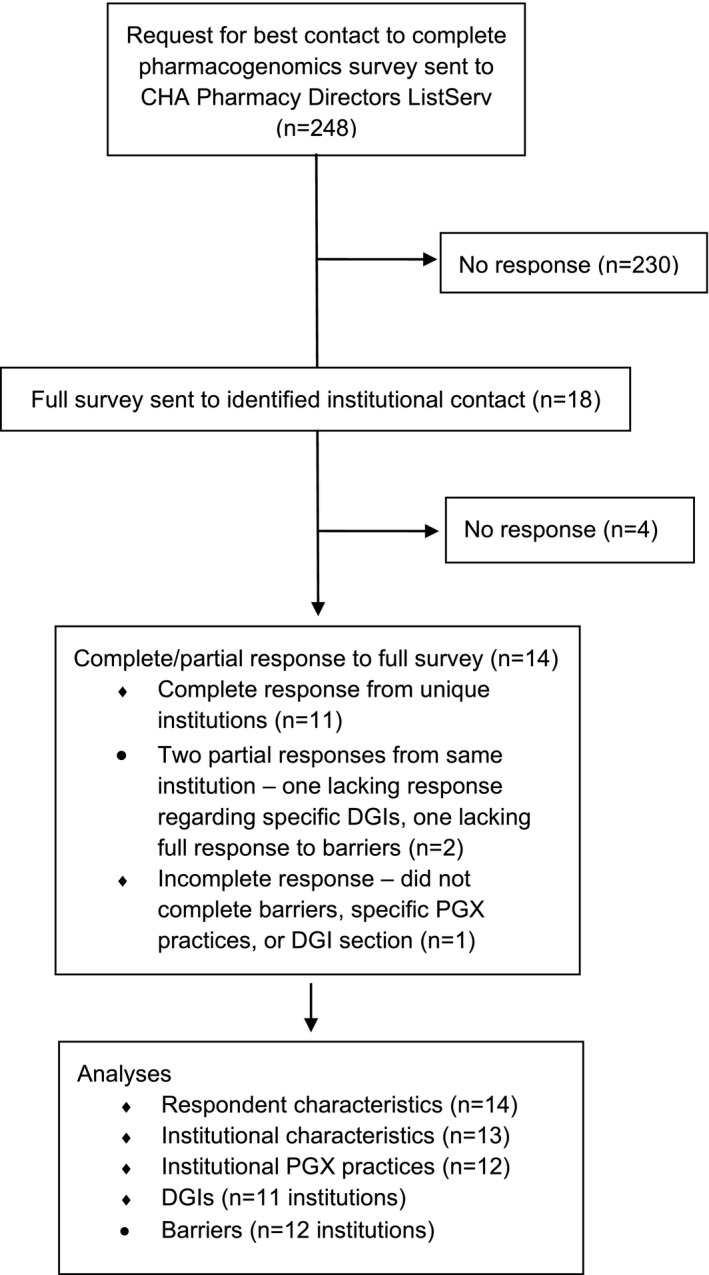
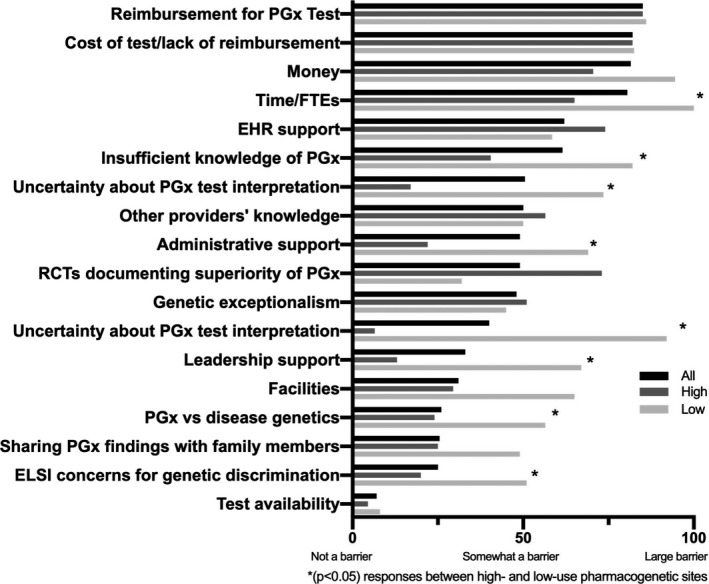
Although pharmacogenetic testing is becoming increasingly common across medical subspecialties, a broad range of utilization and implementation exists across pediatric centers. Large pediatric institutions that routinely use pharmacogenetics in their patient care have published their practices and experiences; however, minimal data exist regarding the full spectrum of pharmacogenetic implementation among children's hospitals. The primary objective of this nationwide survey was to characterize the availability, concerns, and barriers to pharmacogenetic testing in children's hospitals in the Children's Hospital Association. Initial responses identifying a contact person were received from 18 institutions. Of those 18 institutions, 14 responses (11 complete and 3 partial) to a more detailed survey regarding pharmacogenetic practices were received. The majority of respondents were from urban institutions (72%) and held a Doctor of Pharmacy degree (67%). Among all respondents, the three primary barriers to implementing pharmacogenetic testing identified were test reimbursement, test cost, and money. Conversely, the three least concerning barriers were potential for genetic discrimination, sharing results with family members, and availability of tests in certified laboratories. Low-use sites rated several barriers significantly higher than the high-use sites, including knowledge of pharmacogenetics (P = 0.03), pharmacogenetic interpretations (P = 0.04), and pharmacogenetic-based changes to therapy (P = 0.03). In spite of decreasing costs of pharmacogenetic testing, financial barriers are one of the main barriers perceived by pediatric institutions attempting clinical implementation. Low-use sites may also benefit from education/outreach in order to reduce perceived barriers to implementation.
© 2020 The Authors. Clinical and Translational Science published by Wiley Periodicals LLC on behalf of the American Society for Clinical Pharmacology and Therapeutics.
Conflict of interest statement
L.B.R. has received research support from BTG, and International Ltd. All other authors declared no competing interests for this work.
Figures


References
MeSH terms
LinkOut - more resources
Full Text Sources
