

A Pilot Randomized Trial of an Interactive Web-based Tool to Support Surrogate Decision Makers in the Intensive Care Unit
- PMID: 33326348
- PMCID: PMC8328375
- DOI: 10.1513/AnnalsATS.202006-585OC
A Pilot Randomized Trial of an Interactive Web-based Tool to Support Surrogate Decision Makers in the Intensive Care Unit
Abstract
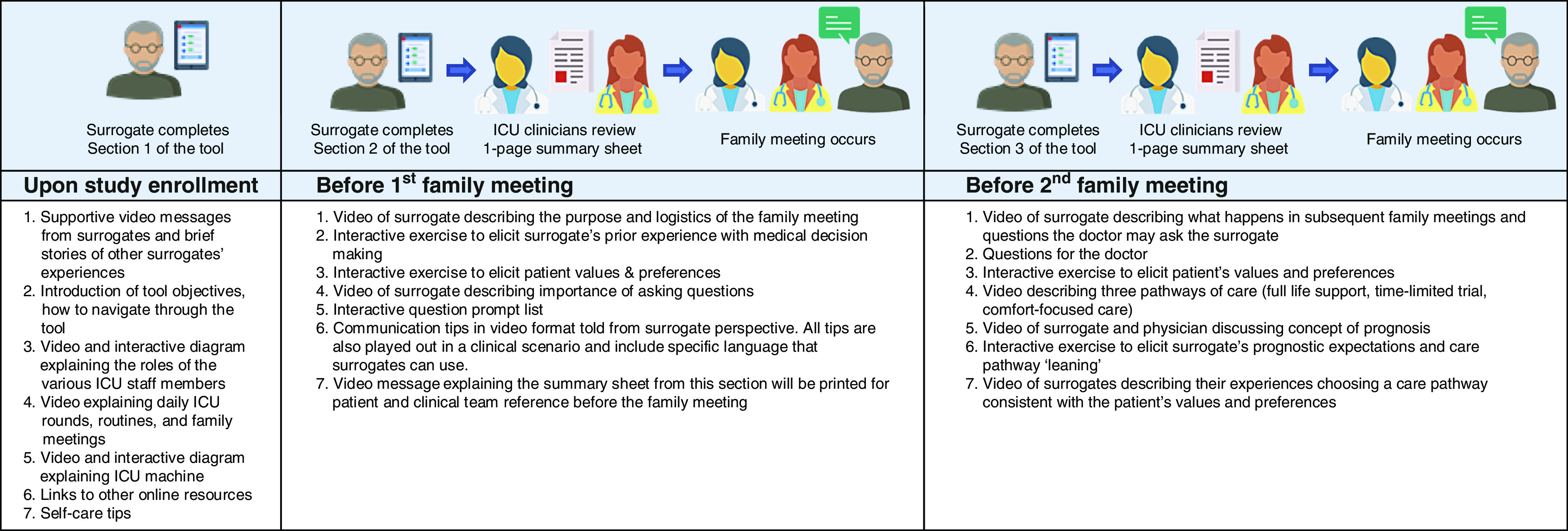
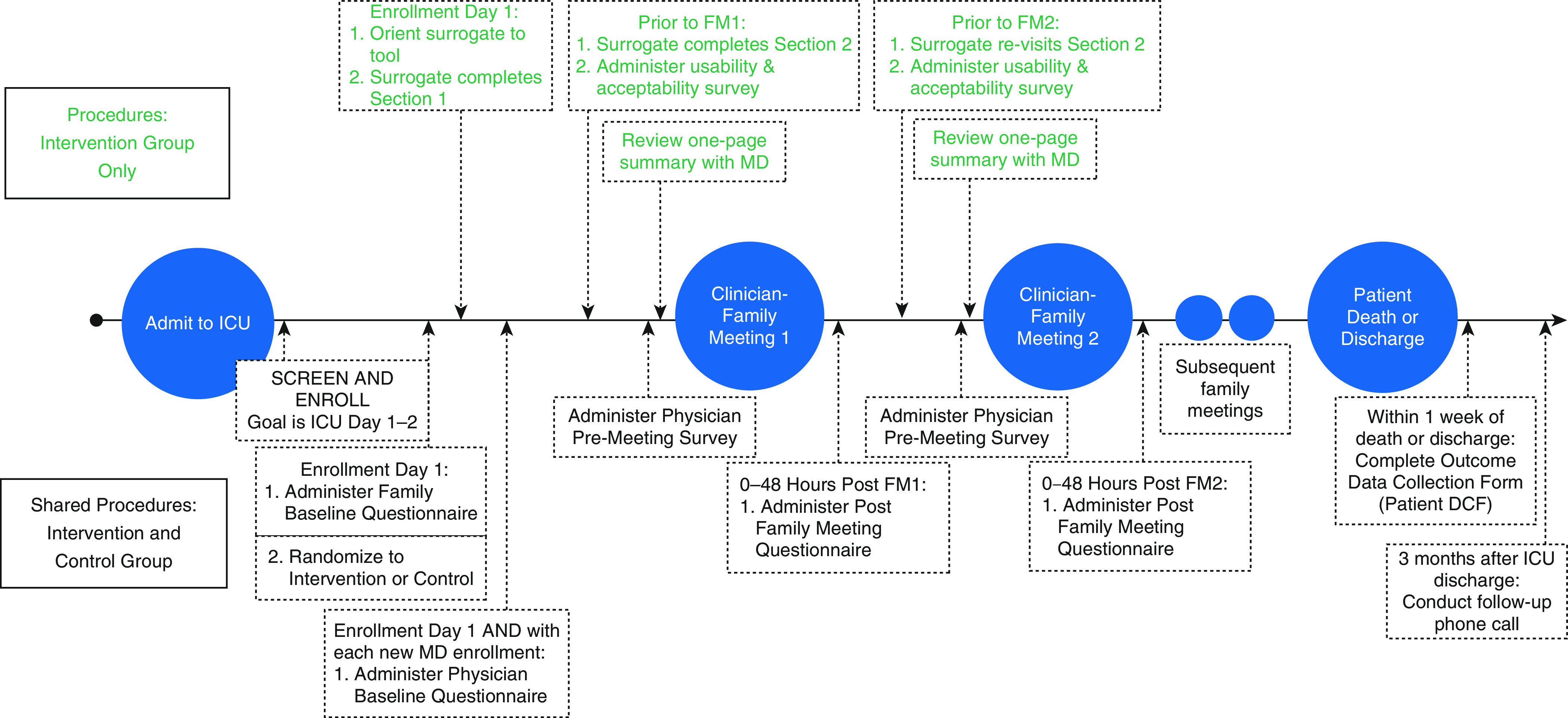
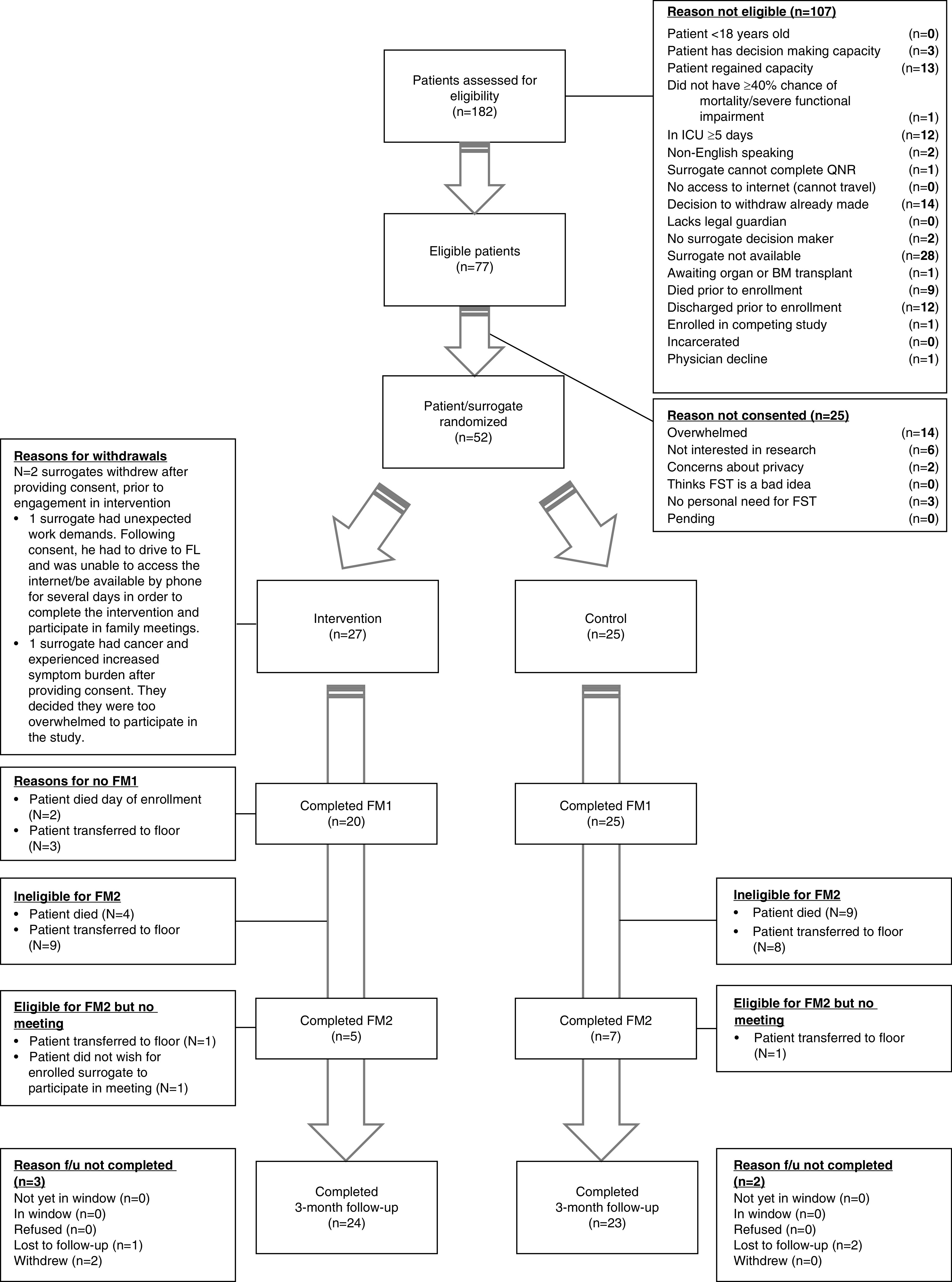
Rationale: Breakdowns in clinician-family communication in intensive care units (ICUs) are common, yet there are no easily scaled interventions to prevent this problem.Objectives: To assess the feasibility, usability, acceptability, and perceived effectiveness of a communication intervention that pairs proactive family meetings with an interactive, web-based tool to help surrogates prepare for clinician-family meetings.Methods: We conducted a two-arm, single-blind, patient-level randomized trial comparing the Family Support Tool with enhanced usual care in two ICUs in a tertiary-care hospital. Eligible participants included surrogates of incapacitated patients judged by their physicians to have ≥40% risk of death or severe long-term functional impairment. The intervention group received unlimited tool access, with prompts to complete specific content upon enrollment and before two scheduled family meetings. Before family meetings, research staff shared with clinicians a one-page summary of surrogates' main questions, prognostic expectations, beliefs about the patient's values, and attitudes about goals of care. The comparator group received usual care enhanced with scheduled family meetings. Feasibility outcomes included the proportion of participants who accessed the tool before the first family meeting, mean number of logins, and average tool engagement time. We assessed tool usability with the System Usability Scale, assessed tool acceptability and perceived effectiveness with internally developed questionnaires, and assessed quality of communication and shared decision-making using the Quality of Communication questionnaire.Results: Of 182 screened patients, 77 were eligible. We enrolled 52 (67.5%) patients and their primary surrogate. Ninety-six percent of intervention surrogates (24/25) accessed the tool before the first family meeting (mean engagement time, 62 min ± 27.7) and logged in 4.2 times (±2.1) on average throughout the hospitalization. Surrogates reported that the tool was highly usable (mean, 82.4/100), acceptable (mean, 4.5/5 ± 0.9), and effective (mean, 4.4/5 ± 0.2). Compared with the control group, surrogates who used the tool reported higher overall quality of communication (mean, 8.9/10 ± 1.6 vs. 8.0/10 ± 2.4) and higher quality in shared decision-making (mean, 8.7/10 ± 1.5 vs. 8.0/10 ± 2.4), but the difference did not reach statistical significance.Conclusions: It is feasible to deploy an interactive web-based tool to support communication and shared decision-making for surrogates in ICUs. Surrogates and clinicians rated the tool as highly usable, acceptable, and effective.
Keywords: clinical trials; communication; critical care; decision-making; internet-based intervention.
Figures
References
-
- Raymont V, Bingley W, Buchanan A, David AS, Hayward P, Wessely S, et al. Prevalence of mental incapacity in medical inpatients and associated risk factors: cross-sectional study. Lancet. 2004;364:1421–1427. - PubMed
-
- McAdam JL, Dracup KA, White DB, Fontaine DK, Puntillo KA. Symptom experiences of family members of intensive care unit patients at high risk for dying. Crit Care Med. 2010;38:1078–1085. - PubMed
-
- Teno JM, Clarridge BR, Casey V, Welch LC, Wetle T, Shield R, et al. Family perspectives on end-of-life care at the last place of care. JAMA. 2004;291:88–93. - PubMed
-
- Azoulay E, Pochard F, Kentish-Barnes N, Chevret S, Aboab J, Adrie C, et al. FAMIREA Study Group. Risk of post-traumatic stress symptoms in family members of intensive care unit patients. Am J Respir Crit Care Med. 2005;171:987–994. - PubMed
