

Mapping routine measles vaccination in low- and middle-income countries
- PMID: 33328634
- PMCID: PMC7739806
- DOI: 10.1038/s41586-020-03043-4
Mapping routine measles vaccination in low- and middle-income countries
Abstract
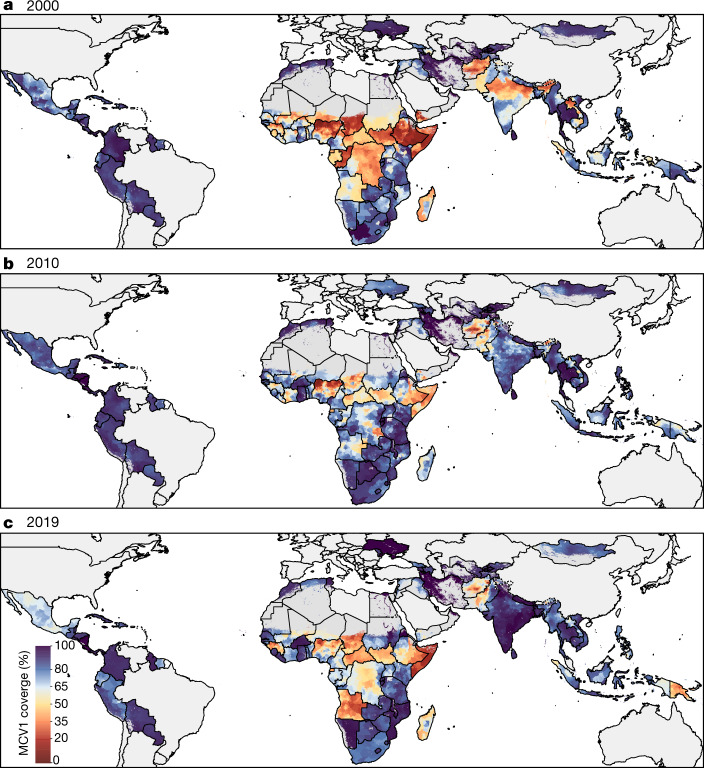
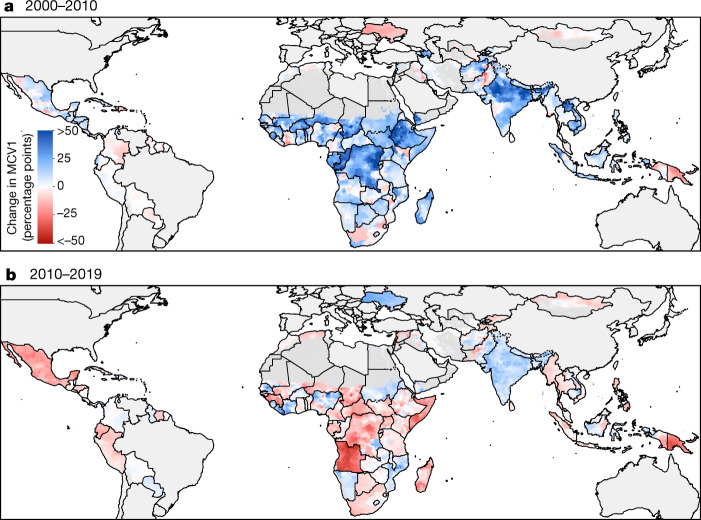
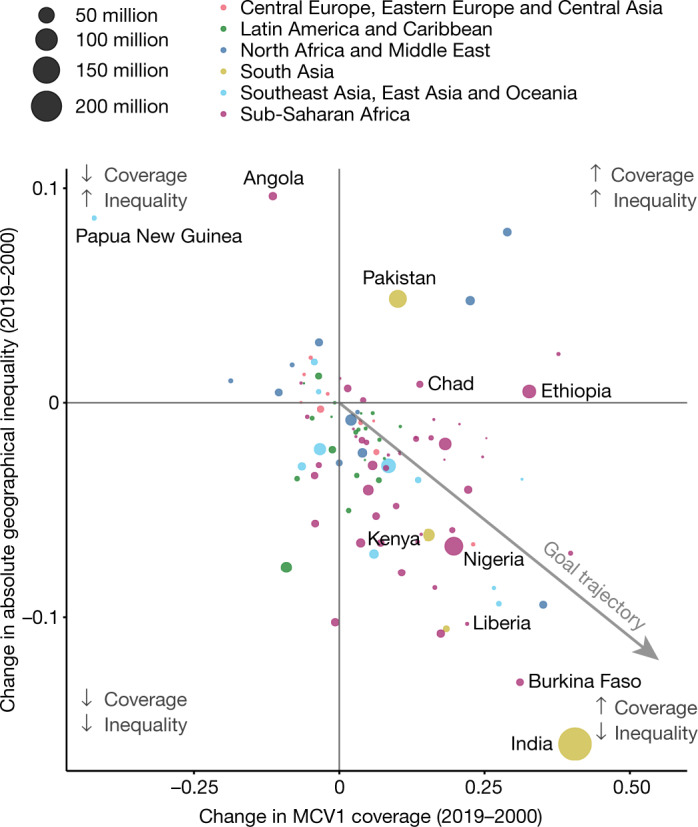
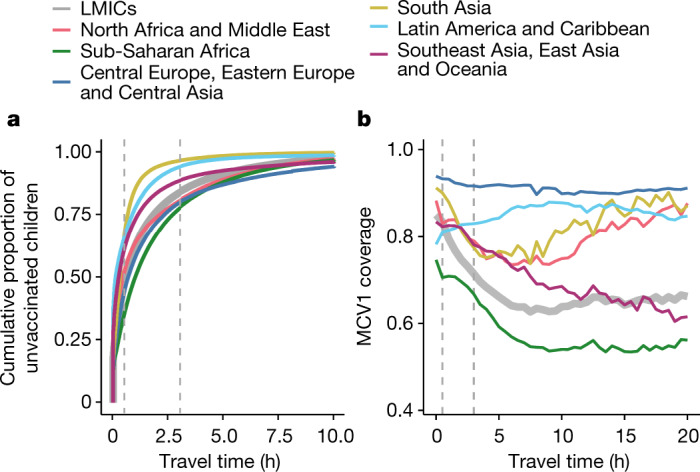
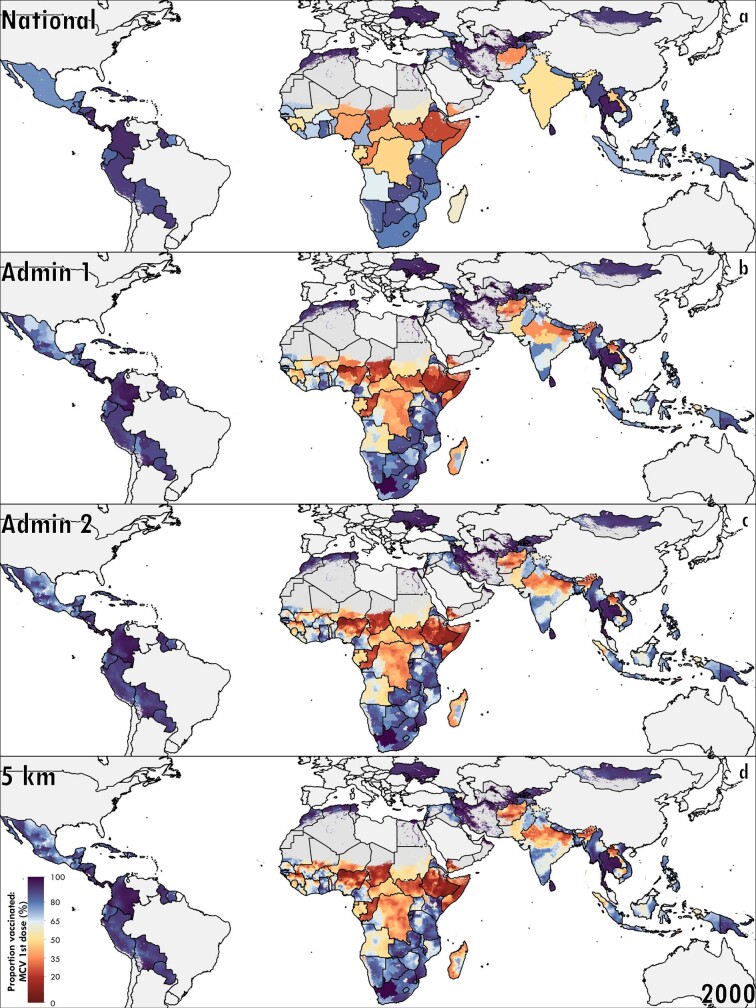
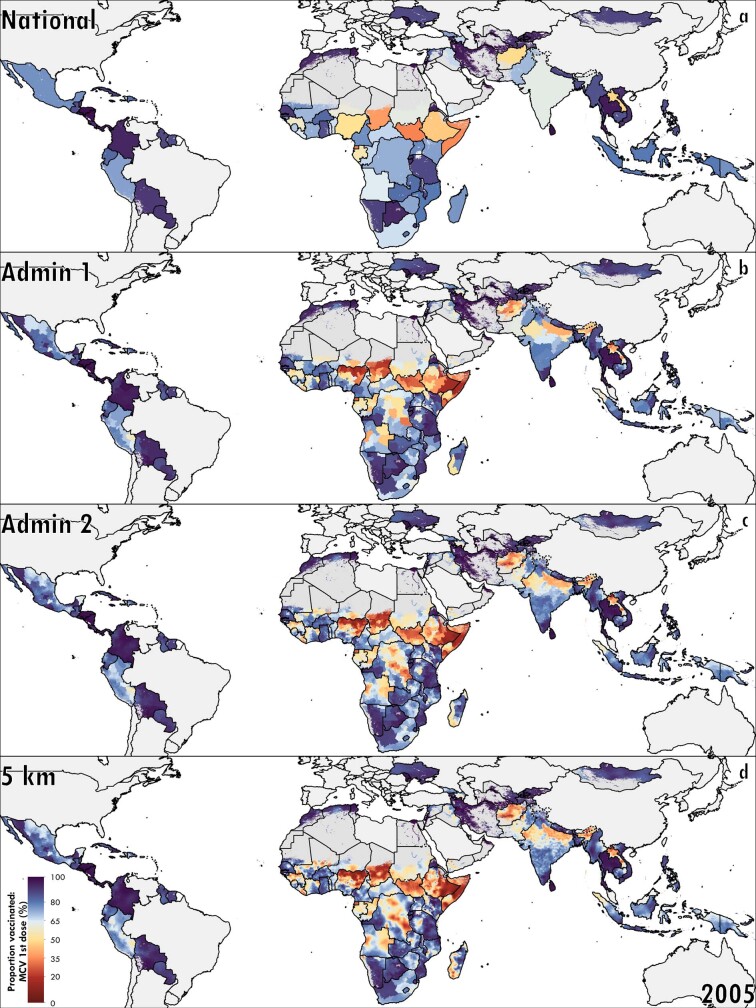
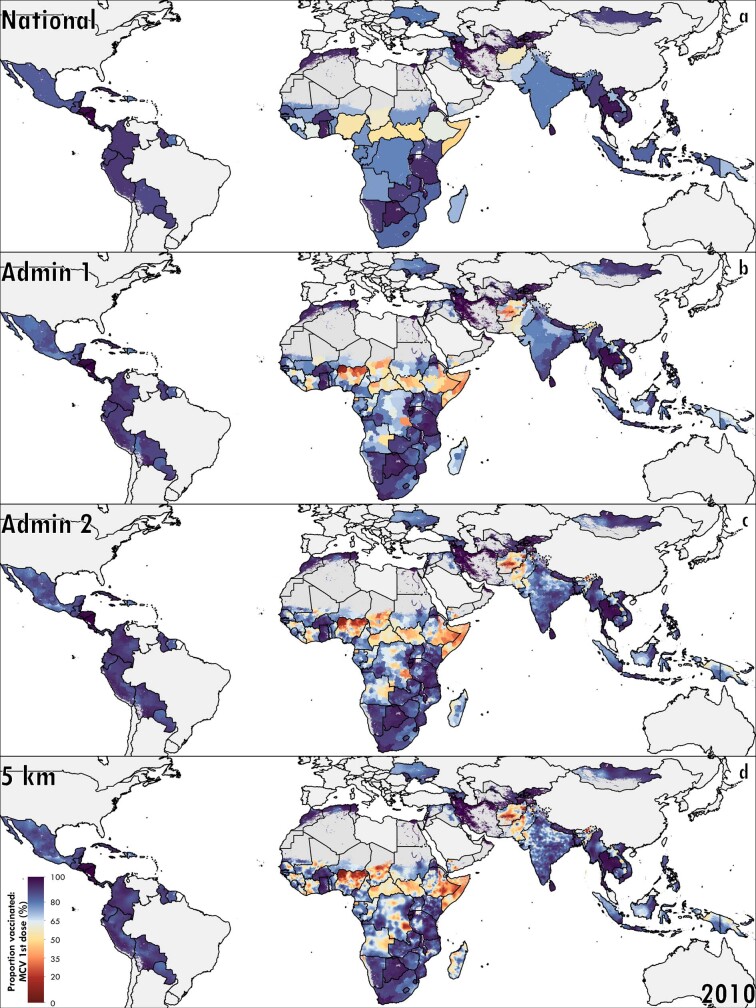
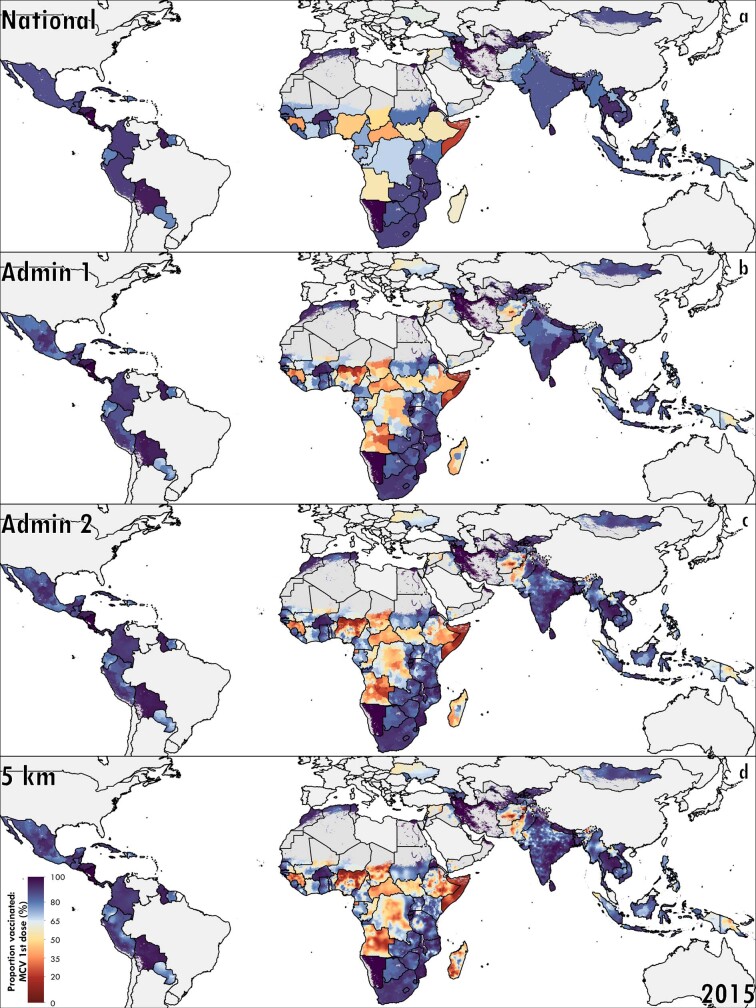
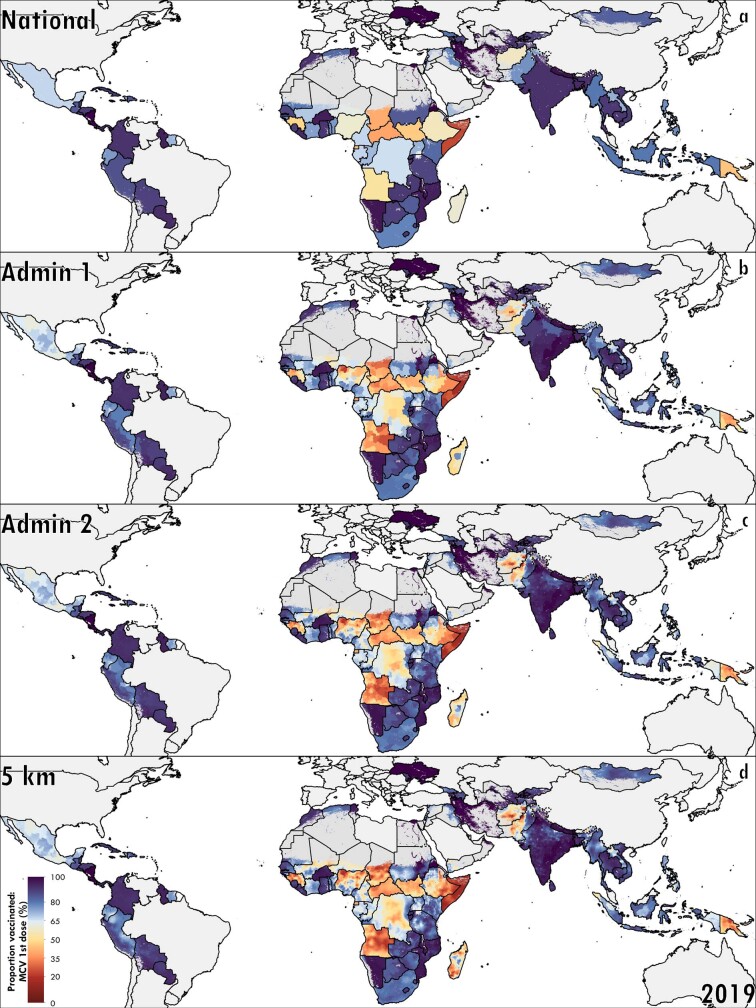
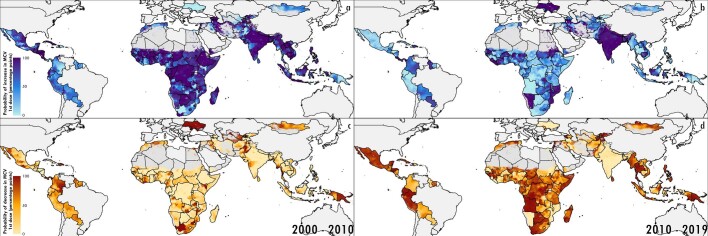
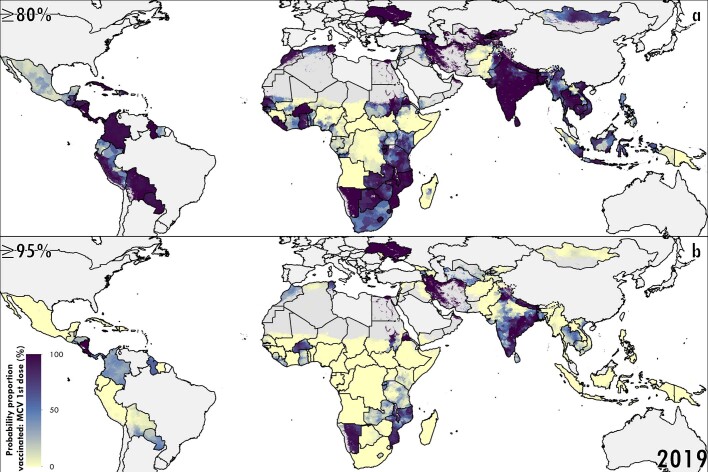
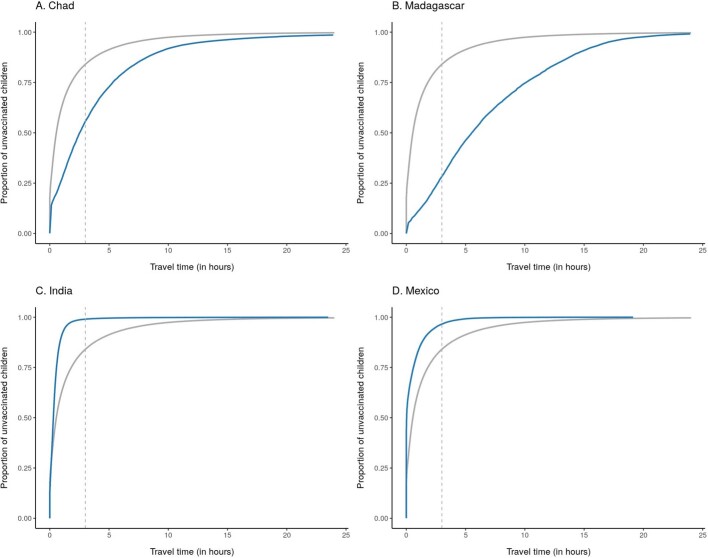
The safe, highly effective measles vaccine has been recommended globally since 1974, yet in 2017 there were more than 17 million cases of measles and 83,400 deaths in children under 5 years old, and more than 99% of both occurred in low- and middle-income countries (LMICs)1-4. Globally comparable, annual, local estimates of routine first-dose measles-containing vaccine (MCV1) coverage are critical for understanding geographically precise immunity patterns, progress towards the targets of the Global Vaccine Action Plan (GVAP), and high-risk areas amid disruptions to vaccination programmes caused by coronavirus disease 2019 (COVID-19)5-8. Here we generated annual estimates of routine childhood MCV1 coverage at 5 × 5-km2 pixel and second administrative levels from 2000 to 2019 in 101 LMICs, quantified geographical inequality and assessed vaccination status by geographical remoteness. After widespread MCV1 gains from 2000 to 2010, coverage regressed in more than half of the districts between 2010 and 2019, leaving many LMICs far from the GVAP goal of 80% coverage in all districts by 2019. MCV1 coverage was lower in rural than in urban locations, although a larger proportion of unvaccinated children overall lived in urban locations; strategies to provide essential vaccination services should address both geographical contexts. These results provide a tool for decision-makers to strengthen routine MCV1 immunization programmes and provide equitable disease protection for all children.
Conflict of interest statement
This study was funded by the Bill & Melinda Gates Foundation. Authors employed by the Bill & Melinda Gates Foundation provided feedback on initial maps and drafts of this manuscript. Otherwise, the funders of the study had no role in study design, data collection, data analysis, data interpretation, or writing of the final report. The corresponding authors had full access to all the data in the study and had final responsibility for the decision to submit for publication. O.O.A. is supported by DSI-NRF Centre of Excellence for Epidemiological Modelling and Analysis (SACEMA). C.A.T.A. reports personal fees from Johnson & Johnson (The Philippines), outside the submitted work. M.L.B. reports grants from the US Environmental Protection Agency, the National Institutes of Health (NIH) and the Wellcome Trust Foundation, during the conduct of the study. M.L.B. also reports honoraria and/or travel reimbursements from the NIH (for the review of grant proposals),
Figures
Comment in
-
Precise mapping reveals gaps in global measles vaccination coverage.Nature. 2021 Jan;589(7842):354-355. doi: 10.1038/d41586-020-03391-1. Nature. 2021. PMID: 33328642 No abstract available.
-
Vaccinate in biodiversity hotspots to protect people and wildlife from each other.Nature. 2021 Mar;591(7850):369. doi: 10.1038/d41586-021-00690-z. Nature. 2021. PMID: 33727722 No abstract available.
-
Disruptions to childhood immunisation due to the COVID-19 pandemic.Lancet. 2021 Aug 7;398(10299):469-471. doi: 10.1016/S0140-6736(21)01418-5. Epub 2021 Jul 17. Lancet. 2021. PMID: 34273290 Free PMC article. No abstract available.
References
-
- McLean HQ, Fiebelkorn AP, Temte JL, Wallace GS. Prevention of measles, rubella, congenital rubella syndrome, and mumps, 2013: summary recommendations of Advisory Committee on Immunization Practices (ACIP) MMWR Morb. Mortal. Wkly Rep. 2013;62:1–34. - PubMed
-
- Keja K, Chan C, Hayden G, Henderson RH. Expanded programme on immunization. World Health Stat. Q. 1988;41:59–63. - PubMed
-
- World Health Assembly. WHO Expanded Programme on Immunization (World Health Organization, 1974).
-
- WHO. Global Vaccine Action Plan 2011–2020. http://www.who.int/immunization/global_vaccine_action_plan/GVAP_doc_2011... (2012).
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
