

Biological Context Linking Hypertension and Higher Risk for COVID-19 Severity
- PMID: 33329052
- PMCID: PMC7710931
- DOI: 10.3389/fphys.2020.599729
Biological Context Linking Hypertension and Higher Risk for COVID-19 Severity
Abstract
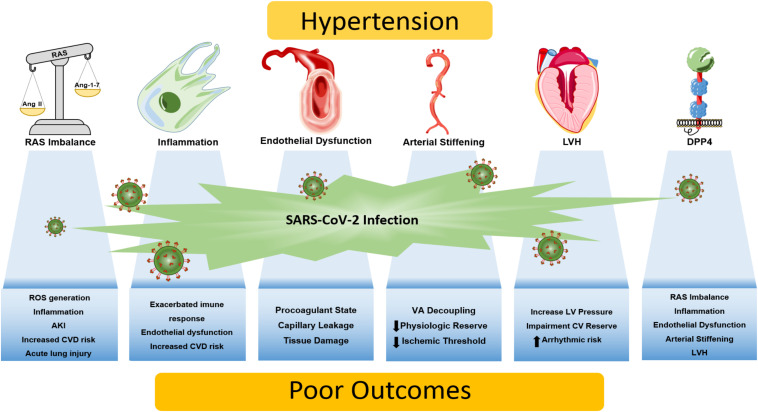
The coronavirus disease 2019 (COVID-19), caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), represents a public health crisis of major proportions. Advanced age, male gender, and the presence of comorbidities have emerged as risk factors for severe illness or death from COVID-19 in observation studies. Hypertension is one of the most common comorbidities in patients with COVID-19. Indeed, hypertension has been shown to be associated with increased risk for mortality, acute respiratory distress syndrome, need for intensive care unit admission, and disease progression in COVID-19 patients. However, up to the present time, the precise mechanisms of how hypertension may lead to the more severe manifestations of disease in patients with COVID-19 remains unknown. This review aims to present the biological plausibility linking hypertension and higher risk for COVID-19 severity. Emphasis is given to the role of the renin-angiotensin system and its inhibitors, given the crucial role that this system plays in both viral transmissibility and the pathophysiology of arterial hypertension. We also describe the importance of the immune system, which is dysregulated in hypertension and SARS-CoV-2 infection, and the potential involvement of the multifunctional enzyme dipeptidyl peptidase 4 (DPP4), that, in addition to the angiotensin-converting enzyme 2 (ACE2), may contribute to the SARS-CoV-2 entrance into target cells. The role of hemodynamic changes in hypertension that might aggravate myocardial injury in the setting of COVID-19, including endothelial dysfunction, arterial stiffness, and left ventricle hypertrophy, are also discussed.
Keywords: COVID; dipeptidyl peptidase 4; hemodynamic factors; hypertension; inflammation; renin-angiotensin system.
Copyright © 2020 Tavares, Bailey and Girardi.
Figures
References
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous