

Extensive Healthy Donor Age/Gender Adjustments and Propensity Score Matching Reveal Physiology of Multiple Sclerosis Through Immunophenotyping
- PMID: 33329307
- PMCID: PMC7732581
- DOI: 10.3389/fneur.2020.565957
Extensive Healthy Donor Age/Gender Adjustments and Propensity Score Matching Reveal Physiology of Multiple Sclerosis Through Immunophenotyping
Abstract
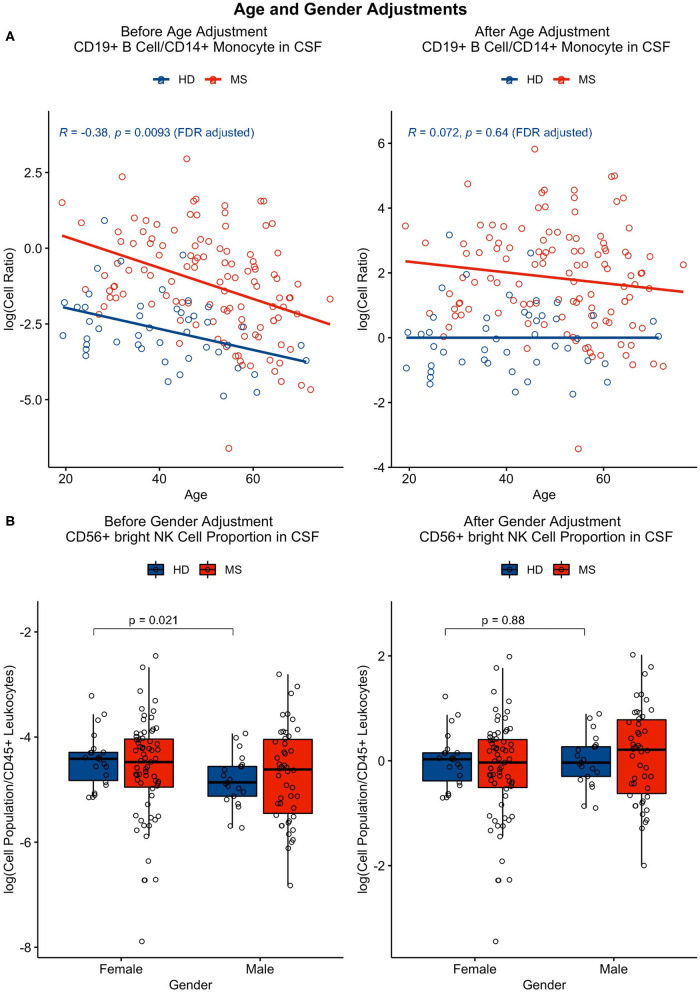
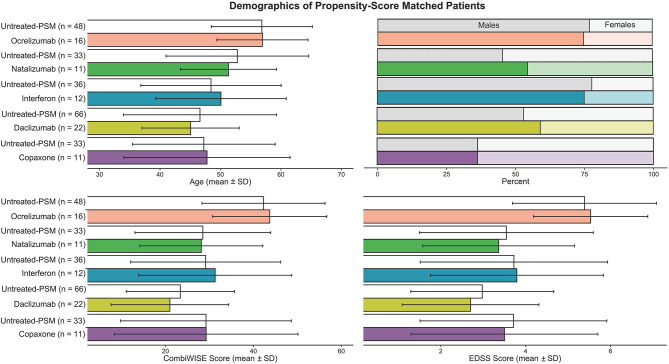
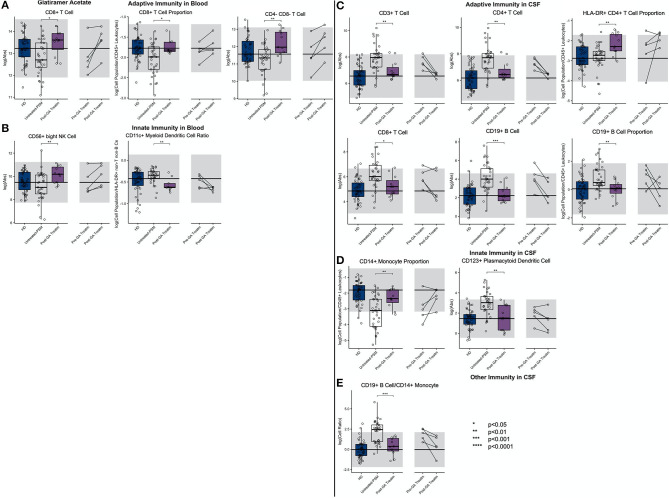
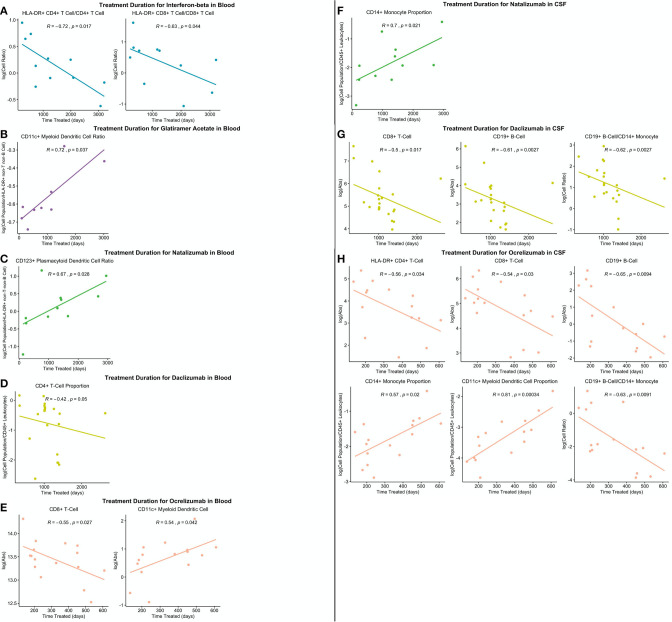
Quantifying cell subpopulations in biological fluids aids in diagnosis and understanding of the mechanisms of injury. Although much has been learned from cerebrospinal fluid (CSF) flow cytometry in neuroimmunological disorders, such as multiple sclerosis (MS), previous studies did not contain enough healthy donors (HD) to derive age- and gender-related normative data and sufficient heterogeneity of other inflammatory neurological disease (OIND) controls to identify MS specific changes. The goals of this blinded training and validation study of MS patients and embedded controls, representing 1,240 prospectively acquired paired CSF/blood samples from 588 subjects was (1) to define physiological age-/gender-related changes in CSF cells, (2) to define/validate cellular abnormalities in blood and CSF of untreated MS through disease duration (DD) and determine which are MS-specific, and (3) to compare effect(s) of low-efficacy (i.e., interferon-beta [IFN-beta] and glatiramer acetate [GA]) and high-efficacy drugs (i.e., natalizumab, daclizumab, and ocrelizumab) on MS-related cellular abnormalities using propensity score matching. Physiological gender differences are less pronounced in the CSF compared to blood, and age-related changes suggest decreased immunosurveillance of CNS by activated HLA-DR+T cells associated with natural aging. Results from patient samples support the concept of MS being immunologically single disease evolving in time. Initially, peripherally activated innate and adaptive immune cells migrate into CSF to form MS lesions. With progression, T cells (CD8+ > CD4+), NK cells, and myeloid dendritic cells are depleted from blood as they continue to accumulate, together with B cells, in the CSF and migrate to CNS tissue, forming compartmentalized inflammation. All MS drugs inhibit non-physiological accumulation of immune cells in the CSF. Although low-efficacy drugs tend to normalize it, high-efficacy drugs overshoot some aspects of CSF physiology, suggesting impairment of CNS immunosurveillance. Comparable inhibition of MS-related CSF abnormalities advocates changes within CNS parenchyma responsible for differences in drug efficacy on MS disability progression. Video summarizing all results may become useful educational tool.
Keywords: age; cerebrospinal fluid; flow cytometry; gender; immunophenotyping; multiple sclerosis; propensity score matching.
Copyright © 2020 Hannikainen, Kosa, Barbour and Bielekova.
Conflict of interest statement
BB is co-inventor on several NIH patents related to daclizumab therapy for MS, and as such, has received patent royalty payments from NIH. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures







Similar articles
-
Daclizumab reverses intrathecal immune cell abnormalities in multiple sclerosis.Ann Clin Transl Neurol. 2015 May;2(5):445-55. doi: 10.1002/acn3.181. Epub 2015 Apr 7. Ann Clin Transl Neurol. 2015. PMID: 26000318 Free PMC article.
-
High interindividual variability in the CD4/CD8 T cell ratio and natalizumab concentration levels in the cerebrospinal fluid of patients with multiple sclerosis.Clin Exp Immunol. 2015 Jun;180(3):383-92. doi: 10.1111/cei.12590. Epub 2015 Apr 27. Clin Exp Immunol. 2015. PMID: 25603898 Free PMC article.
-
Immunophenotyping of cerebrospinal fluid cells in multiple sclerosis: in search of biomarkers.JAMA Neurol. 2014 Jul 1;71(7):905-12. doi: 10.1001/jamaneurol.2014.395. JAMA Neurol. 2014. PMID: 24818670 Review.
-
Comprehensive immunophenotyping of cerebrospinal fluid cells in patients with neuroimmunological diseases.J Immunol. 2014 Mar 15;192(6):2551-63. doi: 10.4049/jimmunol.1302884. Epub 2014 Feb 7. J Immunol. 2014. PMID: 24510966 Free PMC article.
-
Studies on activation variables in multiple sclerosis.Acta Neurol Scand Suppl. 1988;115:1-103. Acta Neurol Scand Suppl. 1988. PMID: 2838999 Review.
Cited by
-
An ANXA11 P93S variant dysregulates TDP-43 and causes corticobasal syndrome.Alzheimers Dement. 2024 Aug;20(8):5220-5235. doi: 10.1002/alz.13915. Epub 2024 Jun 26. Alzheimers Dement. 2024. PMID: 38923692 Free PMC article.
-
Natalizumab Induces Changes of Cerebrospinal Fluid Measures in Multiple Sclerosis.Diagnostics (Basel). 2021 Nov 29;11(12):2230. doi: 10.3390/diagnostics11122230. Diagnostics (Basel). 2021. PMID: 34943468 Free PMC article.
-
How Does Vitamin D Affect Immune Cells Crosstalk in Autoimmune Diseases?Int J Mol Sci. 2023 Feb 28;24(5):4689. doi: 10.3390/ijms24054689. Int J Mol Sci. 2023. PMID: 36902117 Free PMC article. Review.
References
LinkOut - more resources
Full Text Sources
Research Materials