

Upright BPPV Protocol: Feasibility of a New Diagnostic Paradigm for Lateral Semicircular Canal Benign Paroxysmal Positional Vertigo Compared to Standard Diagnostic Maneuvers
- PMID: 33329319
- PMCID: PMC7711159
- DOI: 10.3389/fneur.2020.578305
Upright BPPV Protocol: Feasibility of a New Diagnostic Paradigm for Lateral Semicircular Canal Benign Paroxysmal Positional Vertigo Compared to Standard Diagnostic Maneuvers
Abstract
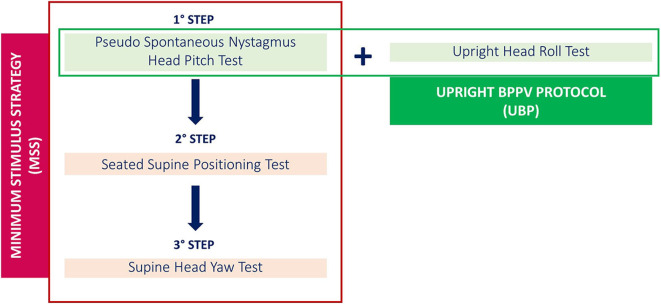
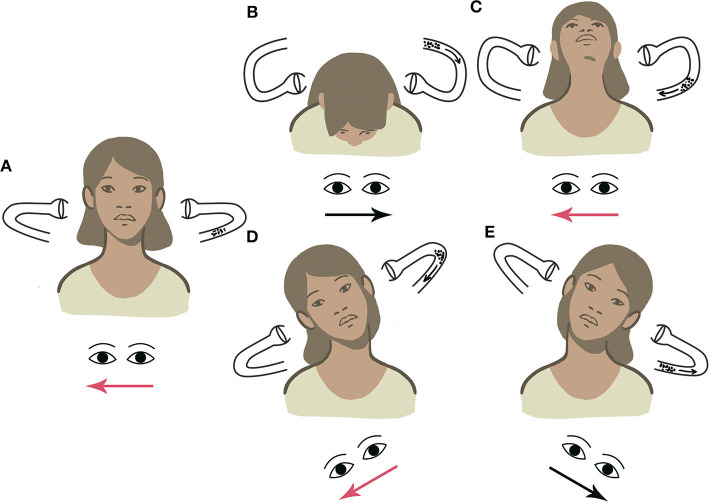
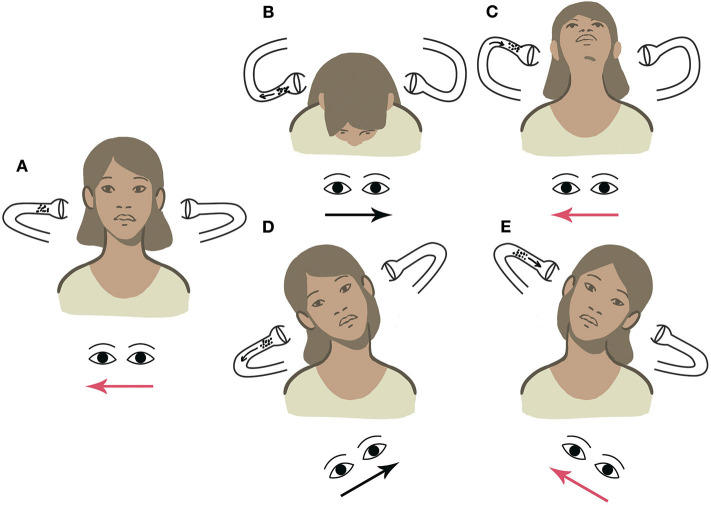
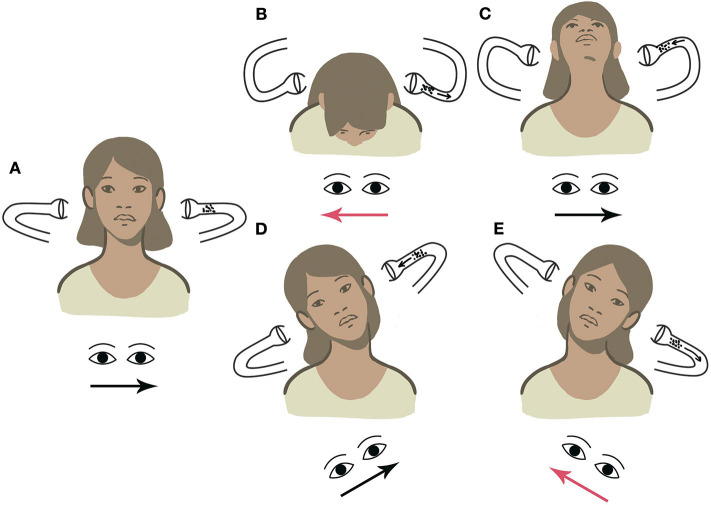
Background: The diagnosis of benign paroxysmal positional vertigo (BPPV) involving the lateral semicircular canal (LSC) is traditionally entrusted to the supine head roll test, also known as supine head yaw test (SHYT), which usually allows identification of the pathologic side and BPPV form (geotropic vs. apogeotropic). Nevertheless, SHYT may not always allow easy detection of the affected canal, resulting in similar responses on both sides and intense autonomic symptoms in patients with recent onset of vertigo. The newly introduced upright head roll test (UHRT) represents a diagnostic maneuver for LSC-BPPV, supplementing the already-known head pitch test (HPT) in the sitting position. The combination of these two tests should enable clinicians to determine the precise location of debris within LSC, avoiding disturbing symptoms related to supine positionings. Therefore, we proposed the upright BPPV protocol (UBP), a test battery exclusively performed in the upright position, including the evaluation of pseudo-spontaneous nystagmus (PSN), HPT and UHRT. The purpose of this multicenter study is to determine the feasibility of UBP in the diagnosis of LSC-BPPV. Methods: We retrospectively reviewed the clinical data of 134 consecutive patients diagnosed with LSC-BPPV. All of them received both UBP and the complete diagnostic protocol (CDP), including the evaluation of PSN and data resulting from HPT, UHRT, seated-supine positioning test (SSPT), and SHYT. Results: A correct diagnosis for LSC-BPPV was achieved in 95.5% of cases using exclusively the UBP, with a highly significant concordance with the CDP (p < 0.000, Cohen's kappa = 0.94), regardless of the time elapsed from symptom onset to diagnosis. The concordance between UBP and CDP was not impaired even when cases in which HPT and/or UHRT provided incomplete results were included (p < 0.000). Correct diagnosis using the supine diagnostic protocol (SDP, including SSPT + SHYT) or the sole SHYT was achieved in 85.1% of cases, with similar statistical concordance (p < 0.000) and weaker strength of relationship (Cohen's kappa = 0.80). Conclusion: UBP allows correct diagnosis in LSC-BPPV from the sitting position in most cases, sparing the patient supine positionings and related symptoms. UBP could also allow clinicians to proceed directly with repositioning maneuvers from the upright position.
Keywords: BPPV; head pitch test; horizontal semicircular canal BPPV; lateral semicircular canal BPPV; upright BPPV protocol; upright head roll test.
Copyright © 2020 Martellucci, Malara, Castellucci, Pecci, Giannoni, Marcelli, Scarpa, Cassandro, Quaglieri, Manfrin, Rebecchi, Armato, Comacchio, Mion, Attanasio, Ralli, Greco, de Vincentiis, Botti, Savoldi, Califano, Ghidini, Pagliuca, Clemenzi, Stolfa, Gallo and Asprella Libonati.
Figures
References
LinkOut - more resources
Full Text Sources