

Neurological Complications and Noninvasive Multimodal Neuromonitoring in Critically Ill Mechanically Ventilated COVID-19 Patients
- PMID: 33329361
- PMCID: PMC7729072
- DOI: 10.3389/fneur.2020.602114
Neurological Complications and Noninvasive Multimodal Neuromonitoring in Critically Ill Mechanically Ventilated COVID-19 Patients
Abstract
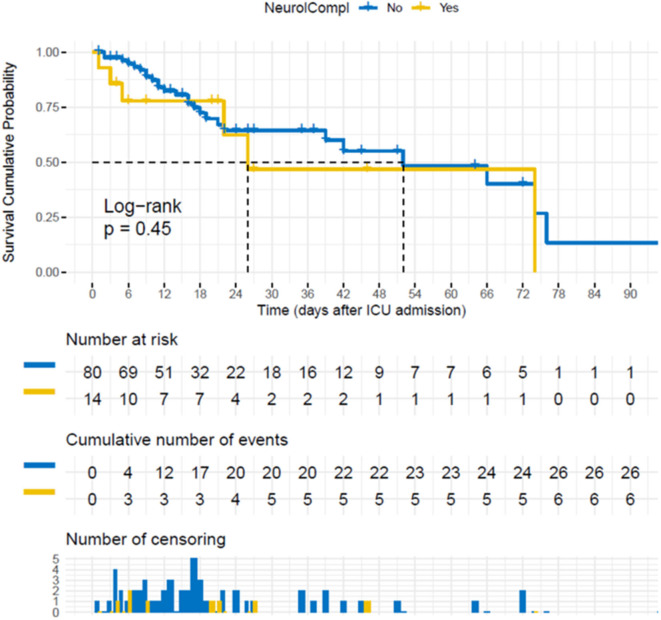
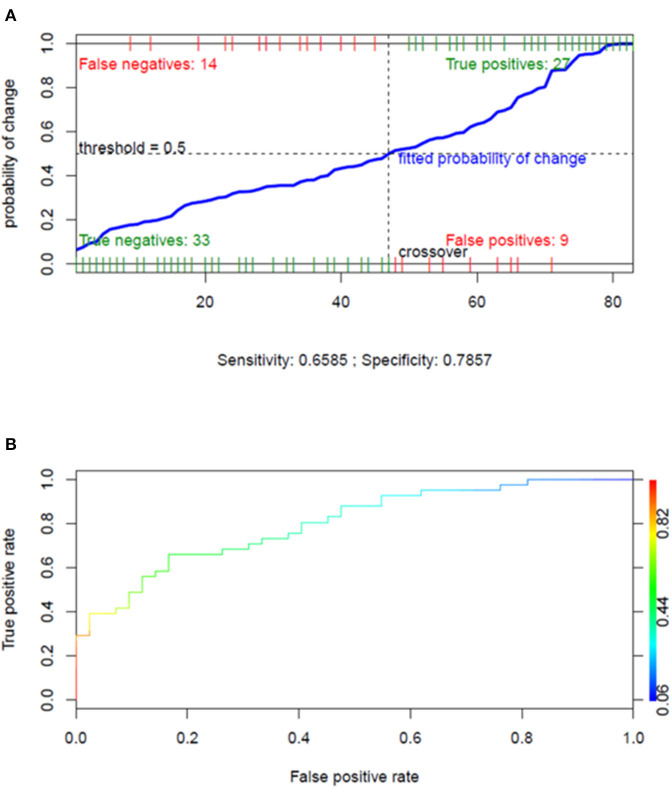
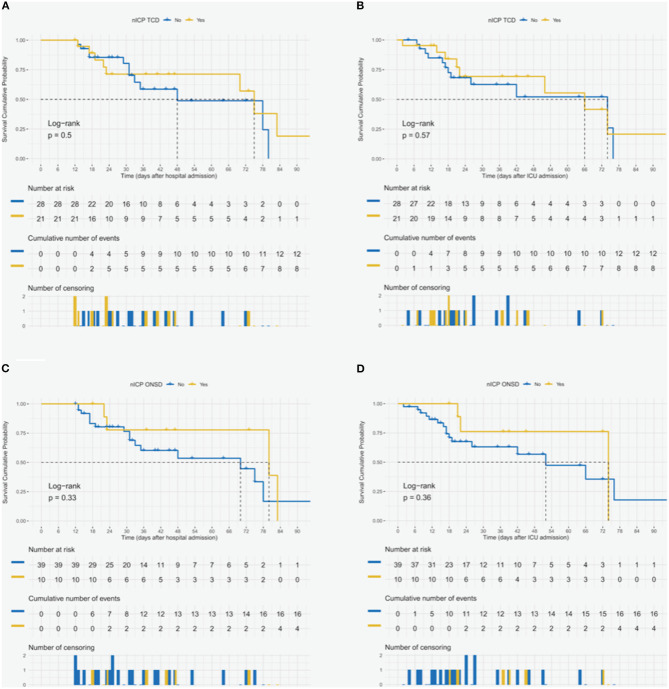
Purpose: The incidence and the clinical presentation of neurological manifestations of coronavirus disease-2019 (COVID-19) remain unclear. No data regarding the use of neuromonitoring tools in this group of patients are available. Methods: This is a retrospective study of prospectively collected data. The primary aim was to assess the incidence and the type of neurological complications in critically ill COVID-19 patients and their effect on survival as well as on hospital and intensive care unit (ICU) length of stay. The secondary aim was to describe cerebral hemodynamic changes detected by noninvasive neuromonitoring modalities such as transcranial Doppler, optic nerve sheath diameter (ONSD), and automated pupillometry. Results: Ninety-four patients with COVID-19 admitted to an ICU from February 28 to June 30, 2020, were included in this study. Fifty-three patients underwent noninvasive neuromonitoring. Neurological complications were detected in 50% of patients, with delirium as the most common manifestation. Patients with neurological complications, compared to those without, had longer hospital (36.8 ± 25.1 vs. 19.4 ± 16.9 days, p < 0.001) and ICU (31.5 ± 22.6 vs. 11.5±10.1 days, p < 0.001) stay. The duration of mechanical ventilation was independently associated with the risk of developing neurological complications (odds ratio 1.100, 95% CI 1.046-1.175, p = 0.001). Patients with increased intracranial pressure measured by ONSD (19% of the overall population) had longer ICU stay. Conclusions: Neurological complications are common in critically ill patients with COVID-19 receiving invasive mechanical ventilation and are associated with prolonged ICU length of stay. Multimodal noninvasive neuromonitoring systems are useful tools for the early detection of variations in cerebrovascular parameters in COVID-19.
Keywords: COVID-19; SARS-CoV-2; neurocritical care; neurological complications; neuromonitoring.
Copyright © 2020 Battaglini, Santori, Chandraptham, Iannuzzi, Bastianello, Tarantino, Ball, Giacobbe, Vena, Bassetti, Inglese, Uccelli, Rocco, Patroniti, Brunetti, Pelosi and Robba.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
LinkOut - more resources
Full Text Sources
Miscellaneous