Comparing hemostatic resuscitation management of intraoperative massive bleeding with traumatic massive bleeding: a computer simulation
- PMID: 33329849
- PMCID: PMC7724118
- DOI: 10.17085/apm.20042
Comparing hemostatic resuscitation management of intraoperative massive bleeding with traumatic massive bleeding: a computer simulation
Abstract
Background: Appropriate blood component transfusion might differ between intraoperative massive bleeding and traumatic massive bleeding in the emergency department because trauma patients initially bleed undiluted blood and replacement typically lags behind blood loss. We compared these two blood loss scenarios, intraoperative and traumatic, using a computer simulation.
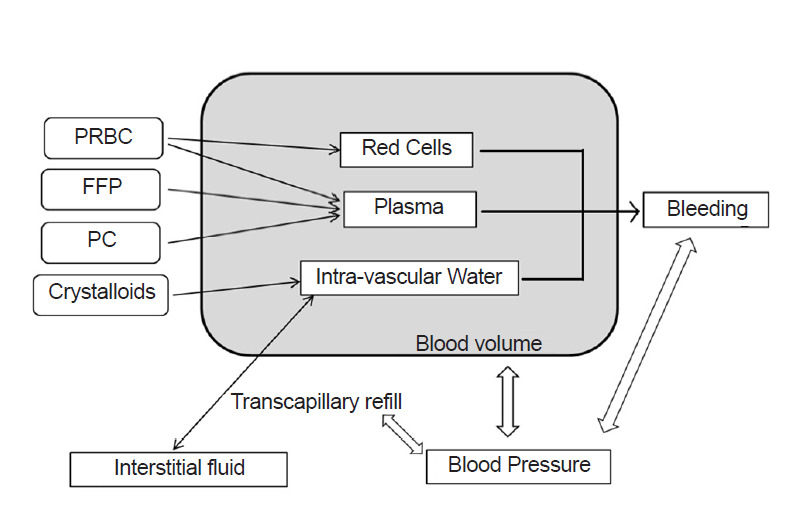
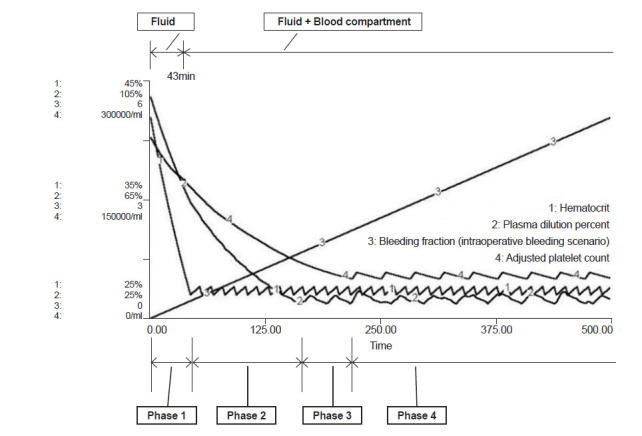
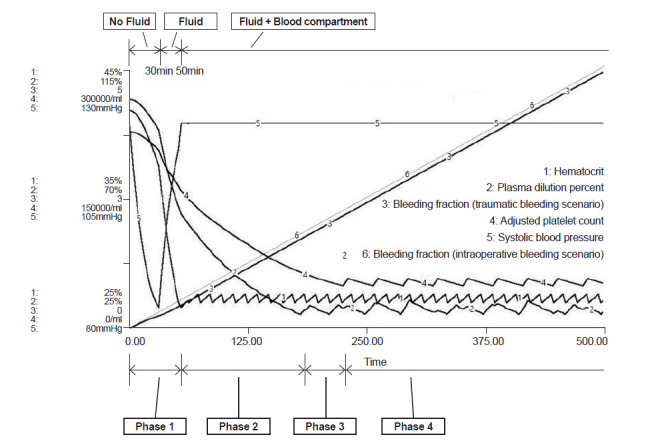
Methods: We modified the multi-compartment dynamic model developed by Hirshberg and implemented it using STELLA 9.0. In this model, blood pressure changes as blood volume fluctuates as bleeding rate and transcapillary refill rate are controlled by blood pressure. Using this simulation, we compared the intraoperative bleeding scenario with the traumatic bleeding scenario. In both scenarios, patients started to bleed at a rate of 50 ml/min. In the intraoperative bleeding scenario, fluid was administered to maintain isovolemic status; however, in the traumatic bleeding scenario, no fluid was supplied for up to 30 min and no blood was supplied for up to 50 min. Each unit of packed red blood cells (PRBC) was given when the hematocrit decreased to 27%, fresh frozen plasma (FFP) was transfused when plasma was diluted to 30%, and platelet concentrate (PC) was transfused when platelet count became 50,000/ml.
Results: In both scenarios, the appropriate ratio of PRBC:FFP was 1:0.47 before PC transfusion, and the ratio of PRBC:FFP:platelets was 1:0.35:0.39 after initiation of PC transfusion.
Conclusion: The ratio of transfused blood component did not differ between the intraoperative bleeding and traumatic bleeding scenarios.
Keywords: Blood coagulation disorder; Blood component transfusion; Computer simulation; Hemorrhage.
Copyright © the Korean Society of Anesthesiologists, 2020.
Conflict of interest statement
CONFLICTS OF INTEREST No potential conflict of interest relevant to this article was reported.
Figures
Similar articles
-
Fresh frozen plasma (FFP) use during massive blood transfusion in trauma resuscitation.Injury. 2010 Jan;41(1):35-9. doi: 10.1016/j.injury.2009.09.029. Injury. 2010. PMID: 19833331
-
Association Between Ratio of Fresh Frozen Plasma to Red Blood Cells During Massive Transfusion and Survival Among Patients Without Traumatic Injury.JAMA Surg. 2017 Jun 1;152(6):574-580. doi: 10.1001/jamasurg.2017.0098. JAMA Surg. 2017. PMID: 28273299 Free PMC article.
-
Hemostatic resuscitation during surgery improves survival in patients with traumatic-induced coagulopathy.J Trauma. 2009 Jul;67(1):33-7; discussion 37-9. doi: 10.1097/TA.0b013e31819adb8e. J Trauma. 2009. PMID: 19590305
-
Hemostatic resuscitation for massive bleeding: the paradigm of plasma and platelets--a review of the current literature.Transfusion. 2010 Mar;50(3):701-10. doi: 10.1111/j.1537-2995.2009.02458.x. Epub 2009 Nov 19. Transfusion. 2010. PMID: 19929864 Review.
-
[Therapy of trauma-induced coagulopathy - what is the evidence?].Anasthesiol Intensivmed Notfallmed Schmerzther. 2012 Sep;47(9):528-39; quiz 540. doi: 10.1055/s-0032-1325284. Epub 2012 Sep 11. Anasthesiol Intensivmed Notfallmed Schmerzther. 2012. PMID: 22968981 Review. German.
References
-
- Guerado E, Medina A, Mata MI, Galvan JM, Bertrand ML. Protocols for massive blood transfusion: when and why, and potential complications. Eur J Trauma Emerg Surg. 2016;42:283–95. - PubMed
-
- Gentilello LM, Pierson DJ. Trauma critical care. Am J Respir Crit Care Med. 2001;163(3 Pt 1):604–7. - PubMed
-
- Cinat ME, Wallace WC, Nastanski F, West J, Sloan S, Ocariz J, et al. Improved survival following massive transfusion in patients who have undergone trauma. Arch Surg. 1999;134:964–8; discussion 968-70. - PubMed
-
- Eddy VA, Morris JA, Jr, Cullinane DC. Hypothermia, coagulopathy, and acidosis. Surg Clin North Am. 2000;80:845–54. - PubMed
LinkOut - more resources
Full Text Sources