

Arterial Stiffness and Hypertension in the Elderly
- PMID: 33330638
- PMCID: PMC7673379
- DOI: 10.3389/fcvm.2020.544302
Arterial Stiffness and Hypertension in the Elderly
Abstract
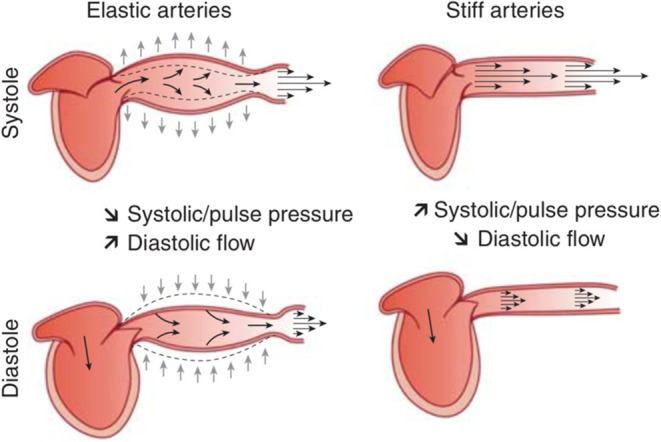
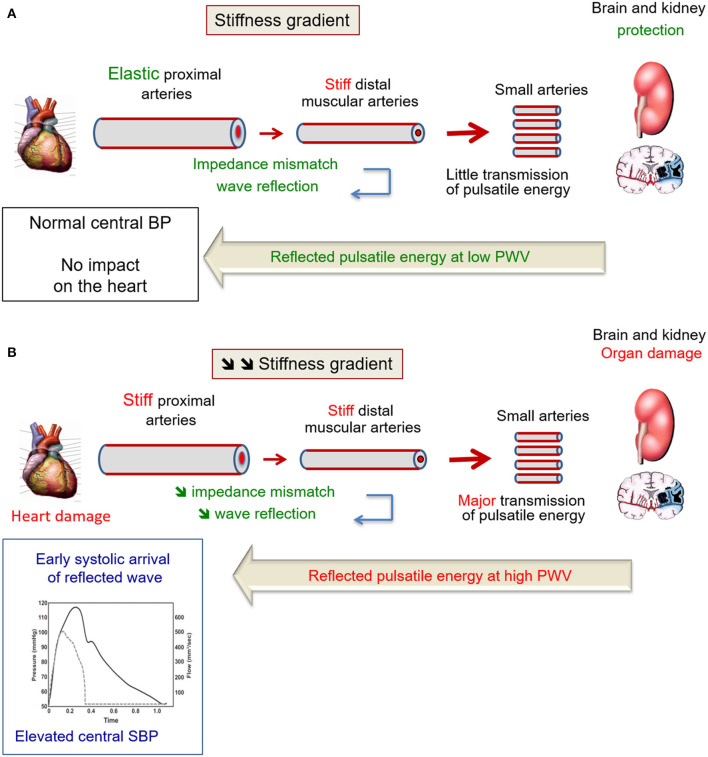
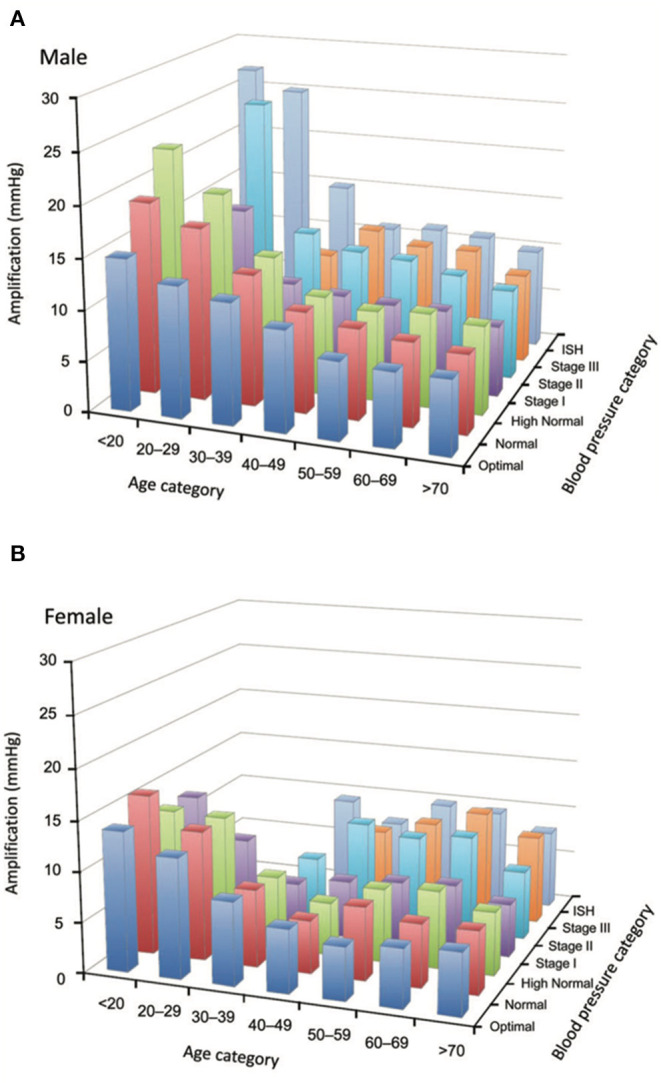
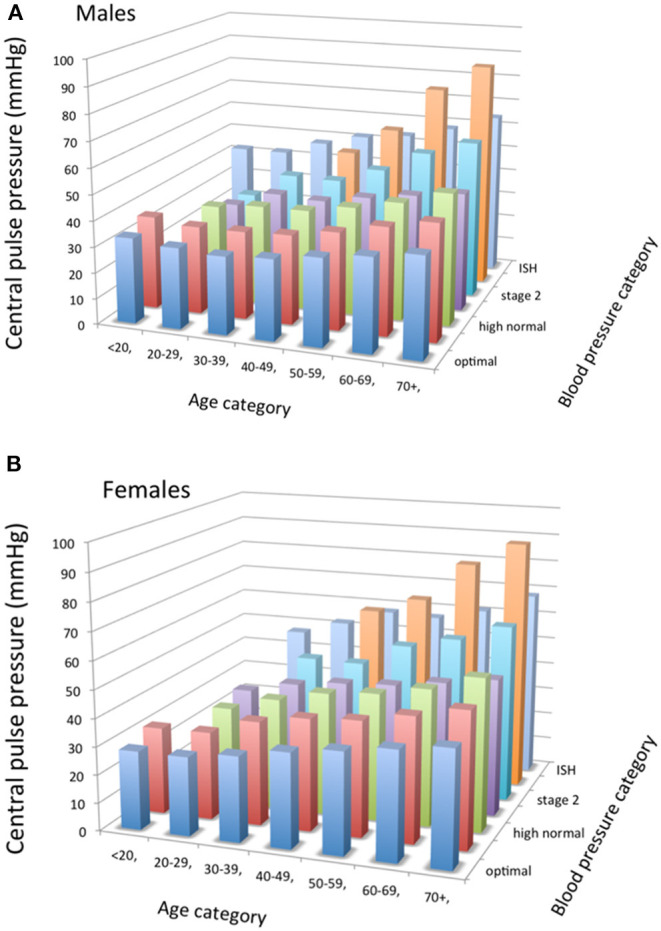
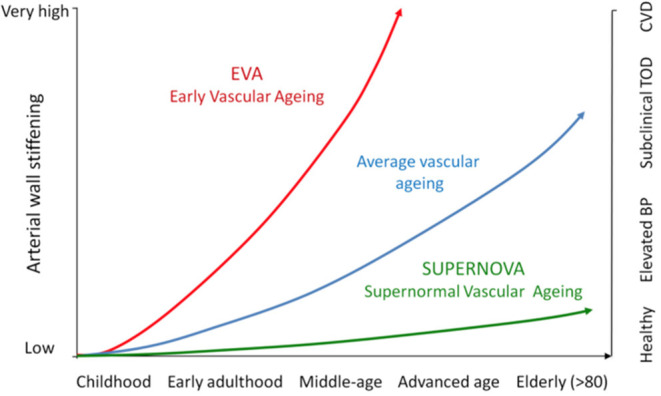
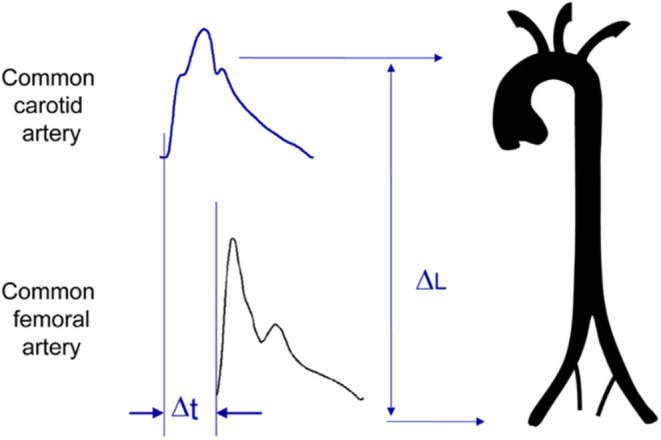
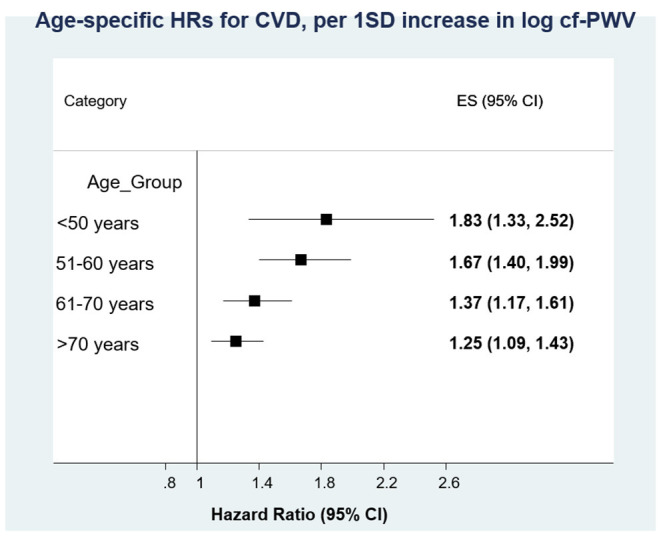
Hypertension prevalence increases with age. Age and high blood pressure are the two main determinants of arterial stiffness. In elderly hypertensives, large arteries stiffen and systolic and pulse pressures increase, due to wave reflections. A major reason for measuring arterial stiffness in clinical practice in elderly hypertensive patients comes from the repeated demonstration that arterial stiffness and wave reflections have a predictive value for CV events. A large body of evidence has been published during the last two decades, concerning the epidemiology, pathophysiology, and pharmacology of large arteries in hypertension in various settings of age. Particularly, two expert consensus documents have reviewed the methodological agreements for measuring arterial stiffness. The concepts of Early Vascular Aging (EVA) and Supernormal Vascular Aging (SUPERNOVA) help to better understand on which determinants of arterial stiffness it is possible to act, in order to limit target organ damage and cardiovascular complications. This review will address the issues of the cellular and molecular mechanisms of arterial stiffening in elderly hypertensives, the consequences of arterial stiffening on central systolic and pulse (systolic minus diastolic, PP) pressures and target organs, the methodology for measuring arterial stiffness, central pulse pressure and wave reflection, the epidemiological determinants of arterial stiffening in elderly hypertensives, the pharmacology of arterial destiffening, and how the concepts of EVA and SUPERNOVA apply to the detection of organ damage and prevention of CV complications.
Keywords: age; arterial stiffness; cardiovascular events; central blood pressure; elderly; large artery; organ damage.
Copyright © 2020 Laurent and Boutouyrie.
Figures
References
-
- Ben-Shlomo Y, Spears M, Boustred C, May M, Anderson SG, Benjamin EJ, et al. . Aortic pulse wave velocity improves cardiovascular event prediction: an individual participant meta-analysis of prospective observational data from 17,635 subjects. J Am Coll Cardiol. (2014) 63:636–46. 10.1016/j.jacc.2013.09.063 - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous