

Tenofovir nephrotoxicity among Asians living with HIV: review of the literature
- PMID: 33330761
- PMCID: PMC7731346
- DOI: 10.35772/ghm.2019.01021
Tenofovir nephrotoxicity among Asians living with HIV: review of the literature
Abstract
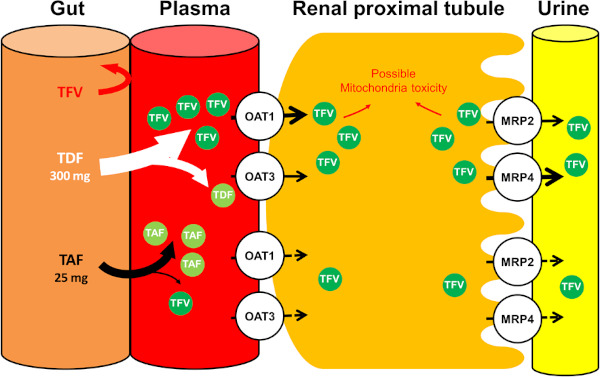
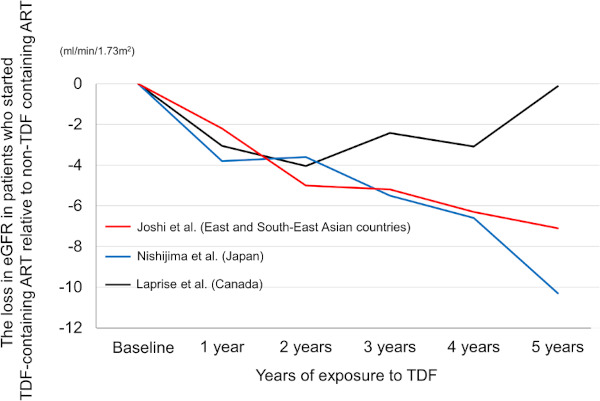
Tenofovir disoproxil fumarate (TDF), prodrug of tenofovir (TFV), is one of the most widely used nucleotide reverse transcriptase inhibitors (NRTIs) for the treatment of HIV infection in resource-rich and resource-limited settings with proven efficacy and safety, and also for the treatment of hepatitis B infections. However, TDF can cause renal proximal tubular dysfunction and also reduces estimated glomerular filtration rate (eGFR) more than other NRTIs. To date, TDF-associated renal dysfunction is generally regarded as mild and tolerable. However, it is notable that low body weight is one of the risk factors for TFV nephrotoxicity and that Asians are generally of smaller body stature and can be susceptible to such nephrotoxicity, as shown in several cohort studies. Until tenofovir alafenamide (TAF), another prodrug of TFV with minimal renal toxicity, becomes widely accessible for people living with HIV and replaces TDF, it is warranted that physicians who prescribe TDF have a good understanding of TFV nephrotoxicity. This paper reviews recent literature on TFV nephrotoxicity among people living with HIV especially focusing on Asians who might be susceptible to TFV nephrotoxicity due to their lower body weight and discusses implications for clinical care and future directions.
Keywords: Asians; HIV infection; Tenofovir; nephrotoxicity; tenofovir alafenamide; tenofovir disoproxil fumarate.
2019, National Center for Global Health and Medicine.
Figures
References
-
- Ghosn J, Taiwo B, Seedat S, Autran B, Katlama C. HIV. Lancet. 2018; 392:685-697. - PubMed
-
- Choi AI, Rodriguez RA, Bacchetti P, Bertenthal D, Volberding PA, O'Hare AM. The impact of HIV on chronic kidney disease outcomes. Kidney Int. 2007; 72:1380-1387. - PubMed
-
- Panel on Antiretroviral Guidelines for Adults and Adolescents. Guidelines for the Use of Antiretroviral Agents in Adults and Adolescents with HIV. Department of Health and Human Services. Available at. http://www.aidsinfo.nih.gov/ContentFiles/AdultandAdolescentGL.pdf (Accessed May 13, 2019).
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
