

Catheter ablation or medical therapy to delay progression of atrial fibrillation: the randomized controlled atrial fibrillation progression trial (ATTEST)
- PMID: 33330909
- PMCID: PMC7947582
- DOI: 10.1093/europace/euaa298
Catheter ablation or medical therapy to delay progression of atrial fibrillation: the randomized controlled atrial fibrillation progression trial (ATTEST)
Abstract
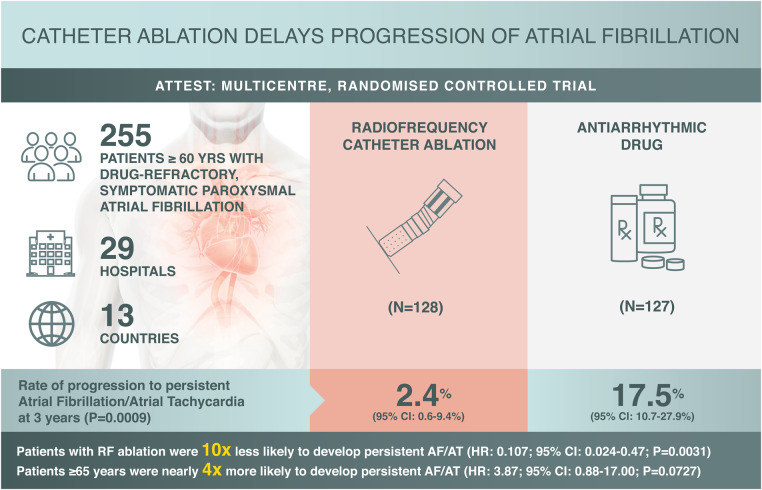
Aims: Delay of progression from paroxysmal to persistent atrial fibrillation (AF) is an important measure of long-term success of AF treatment. However, published data on the impact of catheter ablation on AF progression are limited. This study evaluates whether radiofrequency (RF) catheter ablation delays the progression of AF compared with antiarrhythmic drug (AAD) treatment using current AF management guidelines.
Methods: This prospective, randomized, controlled, two-arm, open-label trial was conducted at 29 hospitals and medical centres across 13 countries. Patients were randomized 1 : 1 to RF ablation or AAD treatment. The primary endpoint was the rate of persistent AF/atrial tachycardia (AT) at 3 years.
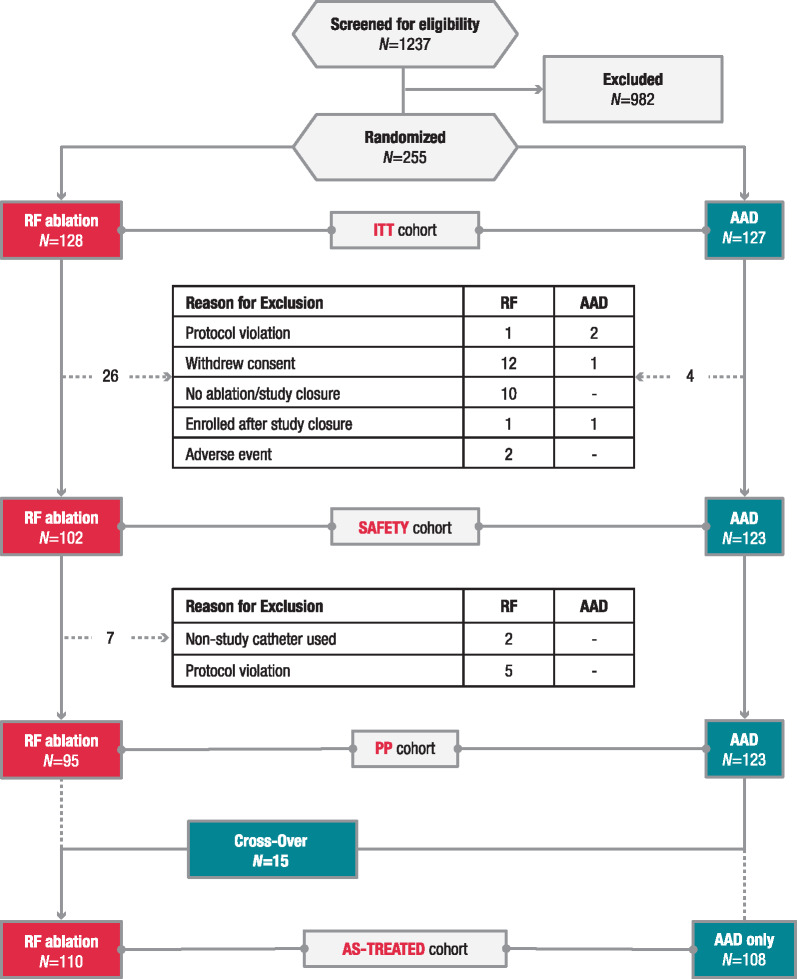
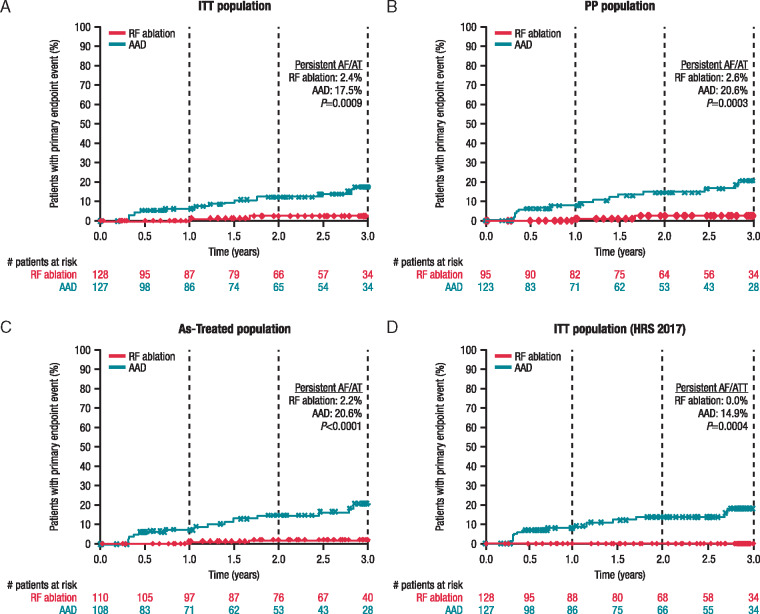
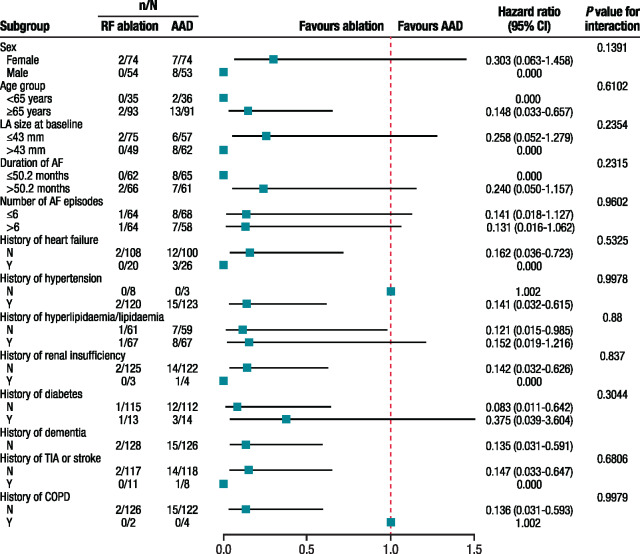
Results: After early study termination following slow enrolment, 255 (79%) of the planned 322 patients were enrolled (RF ablation, n = 128, AAD, n = 127); 36% of patients in the RF ablation group and 41% in the AAD group completed 3 years of follow-up. For the primary endpoint, the Kaplan-Meier estimate of the rate of persistent AF/AT at 3 years was significantly lower with RF ablation [2.4% (95% confidence interval (CI), 0.6-9.4%)] than with AAD therapy [17.5% (95% CI, 10.7-27.9%); one-sided P = 0.0009]. Patients ≥65 years were ∼4 times more likely to progress to persistent AF/AT than patients <65 years, suggesting RF ablation can delay disease progression [hazard ratio: 3.87 (95% CI, 0.88-17.00); P = 0.0727]. Primary adverse events were reported for eight patients in the RF ablation group.
Conclusions: Radiofrequency ablation is superior to guideline-directed AAD therapy in delaying the progression from paroxysmal to persistent AF.
Keywords: Antiarrhythmic drugs; Atrial tachycardia; Persistent atrial fibrillation; Progression; Radiofrequency ablation.
© The Author(s) 2020. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures
References
-
- Chiang CE, Naditch-Brule L, Murin J, Goethals M, Inoue H, O'Neill J. et al. Distribution and risk profile of paroxysmal, persistent, and permanent atrial fibrillation in routine clinical practice: insight from the real-life global survey evaluating patients with atrial fibrillation international registry. Circ Arrhythm Electrophysiol 2012;5:632–9. - PubMed
-
- Ganesan AN, Chew DP, Hartshorne T, Selvanayagam JB, Aylward PE, Sanders P. et al. The impact of atrial fibrillation type on the risk of thromboembolism, mortality, and bleeding: a systematic review and meta-analysis. Eur Heart J 2016;37:1591–602. - PubMed
-
- Cosedis Nielsen J, Johannessen A, Raatikainen P, Hindricks G, Walfridsson H, Kongstad O. et al. Radiofrequency ablation as initial therapy in paroxysmal atrial fibrillation. N Engl J Med 2012;367:1587–95. - PubMed
-
- Nielsen JC, Johannessen A, Raatikainen P, Hindricks G, Walfridsson H, Pehrson SM. et al. Long-term efficacy of catheter ablation as first-line therapy for paroxysmal atrial fibrillation: 5-year outcome in a randomised clinical trial. Heart 2017;103:368–76. - PubMed
-
- Camm AJ, Lip GY, De Caterina R, Savelieva I, Atar D, Hohnloser SH. et al. 2012 focused update of the ESC Guidelines for the management of atrial fibrillation: an update of the 2010 ESC Guidelines for the management of atrial fibrillation. Developed with the special contribution of the European Heart Rhythm Association. Europace 2012;14:1385–413. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
