

Minimally invasive procedure for removal of infected ventriculoatrial shunts
- PMID: 33330950
- PMCID: PMC7815540
- DOI: 10.1007/s00701-020-04675-1
Minimally invasive procedure for removal of infected ventriculoatrial shunts
Abstract
Background: Ventriculoatrial shunts were one of the most common treatments of hydrocephalus in pediatric and adult patients up to about 40 years ago. Thereafter, due to the widespread recognition of the severe cardiac and renal complications associated with ventriculoatrial shunts, they are almost exclusively implanted when other techniques fail. However, late infection or atrial thrombi of previously implanted shunts require removal of the atrial catheter several decades after implantation. Techniques derived from management of central venous access catheters can avoid cardiothoracic surgery in such instances.
Methods: We retrospectively investigated all the patients requiring removal of a VA shunt for complications treated in the last 5 years in our institution.
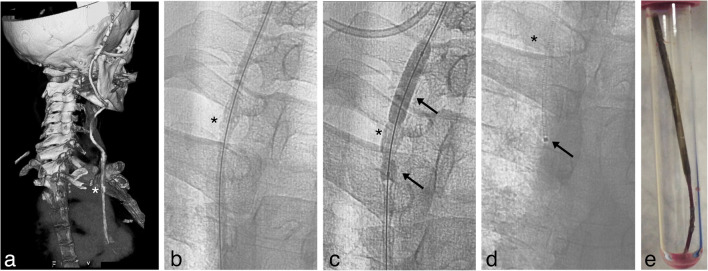
Results: We identified two patients that were implanted 28 and 40 years earlier. Both developed endocarditis with a large atrial thrombus and were successfully treated endovascularly. The successful percutaneous removal was achieved by applying, for the first time in this setting, the endoluminal dilation technique as proposed by Hong. After ventriculoatrial shunt removal and its substitution with an external drainage, both patients where successfully weaned from the need for a shunt and their infection resolved.
Conclusion: Patients carrying a ventriculoatrial shunt are now rarely seen and awareness of long-term ventriculoatrial shunt complications is decreasing. However, these complications must be recognized and treated by shunt removal. Endovascular techniques are appropriate even in the presence of overt endocarditis, atrial thrombi, and tight adherence to the endocardial wall. Moreover, weaning from shunt dependence is possible even decades after shunting.
Keywords: Endocarditis; Endovascular removal; Hydrocephalus; Right atrium; Ventriculoatrial shunt.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures



References
-
- Arze RS, Rashid H, Morley R, Ward MK, Kerr DN. Shunt nephritis: report of two cases and review of the literature. Clin Nephrol. 1983;19(1):48–53. - PubMed
-
- Bastian D, Fessele K, Bednarski P, Göhl K. Interventional laser-assisted extraction of an infected trapped ventriculoatrial shunt based on techniques for pacemaker lead explantation. J Neurol Surg A Cent Eur Neurosurg. 2016;77(01):073–076. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
