

Corrector therapies (with or without potentiators) for people with cystic fibrosis with class II CFTR gene variants (most commonly F508del)
- PMID: 33331662
- PMCID: PMC8094390
- DOI: 10.1002/14651858.CD010966.pub3
Corrector therapies (with or without potentiators) for people with cystic fibrosis with class II CFTR gene variants (most commonly F508del)
Update in
-
Corrector therapies (with or without potentiators) for people with cystic fibrosis with class II CFTR gene variants (most commonly F508del).Cochrane Database Syst Rev. 2023 Nov 20;11(11):CD010966. doi: 10.1002/14651858.CD010966.pub4. Cochrane Database Syst Rev. 2023. PMID: 37983082 Free PMC article.
Abstract
Background: Cystic fibrosis (CF) is a common life-shortening genetic condition caused by a variant in the cystic fibrosis transmembrane conductance regulator (CFTR) protein. A class II CFTR variant F508del (found in up to 90% of people with CF (pwCF)) is the commonest CF-causing variant. The faulty protein is degraded before reaching the cell membrane, where it needs to be to effect transepithelial salt transport. The F508del variant lacks meaningful CFTR function and corrective therapy could benefit many pwCF. Therapies in this review include single correctors and any combination of correctors and potentiators.
Objectives: To evaluate the effects of CFTR correctors (with or without potentiators) on clinically important benefits and harms in pwCF of any age with class II CFTR mutations (most commonly F508del).
Search methods: We searched the Cochrane Cystic Fibrosis and Genetic Disorders Cystic Fibrosis Trials Register, reference lists of relevant articles and online trials registries. Most recent search: 14 October 2020.
Selection criteria: Randomised controlled trials (RCTs) (parallel design) comparing CFTR correctors to control in pwCF with class II mutations.
Data collection and analysis: Two authors independently extracted data, assessed risk of bias and evidence quality (GRADE); we contacted investigators for additional data.
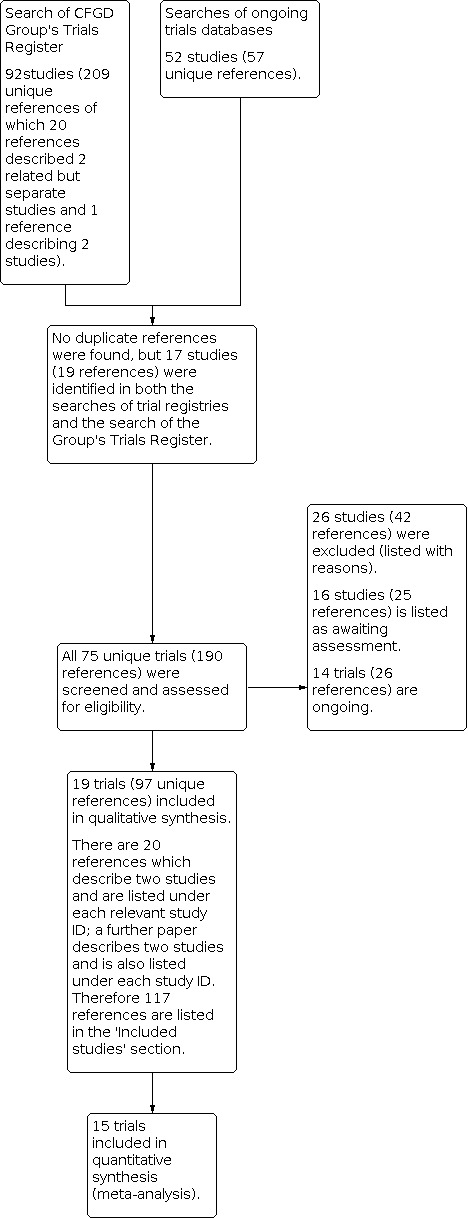
Main results: We included 19 RCTs (2959 participants), lasting between 1 day and 24 weeks; an extension of two lumacaftor-ivacaftor studies provided additional 96-week safety data (1029 participants). We assessed eight monotherapy RCTs (344 participants) (4PBA, CPX, lumacaftor, cavosonstat and FDL169), six dual-therapy RCTs (1840 participants) (lumacaftor-ivacaftor or tezacaftor-ivacaftor) and five triple-therapy RCTs (775 participants) (elexacaftor-tezacaftor-ivacaftor or VX-659-tezacaftor-ivacaftor); below we report only the data from elexacaftor-tezacaftor-ivacaftor combination which proceeded to Phase 3 trials. In 14 RCTs participants had F508del/F508del genotypes, in three RCTs F508del/minimal function (MF) genotypes and in two RCTs both genotypes. Risk of bias judgements varied across different comparisons. Results from 11 RCTs may not be applicable to all pwCF due to age limits (e.g. adults only) or non-standard design (converting from monotherapy to combination therapy). Monotherapy Investigators reported no deaths or clinically-relevant improvements in quality of life (QoL). There was insufficient evidence to determine any important effects on lung function. No placebo-controlled monotherapy RCT demonstrated differences in mild, moderate or severe adverse effects (AEs); the clinical relevance of these events is difficult to assess with their variety and small number of participants (all F508del/F508del). Dual therapy Investigators reported no deaths (moderate- to high-quality evidence). QoL scores (respiratory domain) favoured both lumacaftor-ivacaftor and tezacaftor-ivacaftor therapy compared to placebo at all time points. At six months lumacaftor 600 mg or 400 mg (both once daily) plus ivacaftor improved Cystic Fibrosis Questionnaire (CFQ) scores slightly compared with placebo (mean difference (MD) 2.62 points (95% confidence interval (CI) 0.64 to 4.59); 1061 participants; high-quality evidence). A similar effect was observed for twice-daily lumacaftor (200 mg) plus ivacaftor (250 mg), but with low-quality evidence (MD 2.50 points (95% CI 0.10 to 5.10)). The mean increase in CFQ scores with twice-daily tezacaftor (100 mg) and ivacaftor (150 mg) was approximately five points (95% CI 3.20 to 7.00; 504 participants; moderate-quality evidence). At six months, the relative change in forced expiratory volume in one second (FEV1) % predicted improved with combination therapies compared to placebo by: 5.21% with once-daily lumacaftor-ivacaftor (95% CI 3.61% to 6.80%; 504 participants; high-quality evidence); 2.40% with twice-daily lumacaftor-ivacaftor (95% CI 0.40% to 4.40%; 204 participants; low-quality evidence); and 6.80% with tezacaftor-ivacaftor (95% CI 5.30 to 8.30%; 520 participants; moderate-quality evidence). More pwCF reported early transient breathlessness with lumacaftor-ivacaftor, odds ratio 2.05 (99% CI 1.10 to 3.83; 739 participants; high-quality evidence). Over 120 weeks (initial study period and follow-up) systolic blood pressure rose by 5.1 mmHg and diastolic blood pressure by 4.1 mmHg with twice-daily 400 mg lumacaftor-ivacaftor (80 participants; high-quality evidence). The tezacaftor-ivacaftor RCTs did not report these adverse effects. Pulmonary exacerbation rates decreased in pwCF receiving additional therapies to ivacaftor compared to placebo: lumacaftor 600 mg hazard ratio (HR) 0.70 (95% CI 0.57 to 0.87; 739 participants); lumacaftor 400 mg, HR 0.61 (95% CI 0.49 to 0.76; 740 participants); and tezacaftor, HR 0.64 (95% CI, 0.46 to 0.89; 506 participants) (moderate-quality evidence). Triple therapy Three RCTs of elexacaftor to tezacaftor-ivacaftor in pwCF (aged 12 years and older with either one or two F508del variants) reported no deaths (high-quality evidence). All other evidence was graded as moderate quality. In 403 participants with F508del/minimal function (MF) elexacaftor-tezacaftor-ivacaftor improved QoL respiratory scores (MD 20.2 points (95% CI 16.2 to 24.2)) and absolute change in FEV1 (MD 14.3% predicted (95% CI 12.7 to 15.8)) compared to placebo at 24 weeks. At four weeks in 107 F508del/F508del participants, elexacaftor-tezacaftor-ivacaftor improved QoL respiratory scores (17.4 points (95% CI 11.9 to 22.9)) and absolute change in FEV1 (MD 10.0% predicted (95% CI 7.5 to 12.5)) compared to tezacaftor-ivacaftor. There was probably little or no difference in the number or severity of AEs between elexacaftor-tezacaftor-ivacaftor and placebo or control (moderate-quality evidence). In 403 F508del/F508del participants, there was a longer time to protocol-defined pulmonary exacerbation with elexacaftor-tezacaftor-ivacaftor over 24 weeks (moderate-quality evidence).
Authors' conclusions: There is insufficient evidence that corrector monotherapy has clinically important effects in pwCF with F508del/F508del. Both dual therapies (lumacaftor-ivacaftor, tezacaftor-ivacaftor) result in similar improvements in QoL and respiratory function with lower pulmonary exacerbation rates. Lumacaftor-ivacaftor was associated with an increase in early transient shortness of breath and longer-term increases in blood pressure (not observed for tezacaftor-ivacaftor). Tezacaftor-ivacaftor has a better safety profile, although data are lacking in children under 12 years. In this population, lumacaftor-ivacaftor had an important impact on respiratory function with no apparent immediate safety concerns; but this should be balanced against the blood pressure increase and shortness of breath seen in longer-term adult data when considering lumacaftor-ivacaftor. There is high-quality evidence of clinical efficacy with probably little or no difference in AEs for triple (elexacaftor-tezacaftor-ivacaftor) therapy in pwCF with one or two F508del variants aged 12 years or older. Further RCTs are required in children (under 12 years) and those with more severe respiratory function.
Trial registration: ClinicalTrials.gov NCT01225211 NCT00865904 NCT03029455 NCT03224351 NCT01746784 NCT03093714 NCT03227471 NCT00004428 NCT01931839 NCT02514473 NCT00590538 NCT01807923 NCT01807949 NCT00016744 NCT01897233 NCT00742092 NCT00945347 NCT01899105 NCT03447262 NCT03525574 NCT03537651 NCT03601637 NCT03633526 NCT03691779 NCT04043806 NCT04058366 NCT04105972 NCT04183790 NCT04235140 NCT04362761 NCT04537793 NCT04545515 NCT02392234 NCT03045523 NCT03559062.
Copyright © 2020 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Conflict of interest statement
Professor Kevin Southern declares no potential conflict of interest.
Dr Ian Sinha is in receipt of a NIHR HTA grant for paediatric asthma and is a member of the NICE asthma committee; however, neither of these are related to cystic fibrosis or this review and thus do not constitute a potential conflict of interest.
Dr Sarah J Nevitt declares no potential conflict of interest.
Dr Jared Murphy declares no potential conflict of interest.
Figures



































































































































































Update of
-
Correctors (specific therapies for class II CFTR mutations) for cystic fibrosis.Cochrane Database Syst Rev. 2018 Aug 2;8(8):CD010966. doi: 10.1002/14651858.CD010966.pub2. Cochrane Database Syst Rev. 2018. Update in: Cochrane Database Syst Rev. 2020 Dec 17;12:CD010966. doi: 10.1002/14651858.CD010966.pub3. PMID: 30070364 Free PMC article. Updated. Review.
References
References to studies included in this review
Boyle 2014 {published data only}2010‐020413‐90
-
- Boyle M, Bell SC, Konstan M, McColley S, Flume P, Kang L, et al. Lumacaftor, an investigational CFTR corrector, in combination with ivacaftor, a CFTR potentiator, in CF patients with the F508del-CFTR mutation: phase 2 interim analysis. Journal of Cystic Fibrosis 2013;12 Suppl 1:S14. [ABSTRACT NO.: WS7.4] [CENTRAL: 921640] [CFGD REGISTER: BD169c]
-
- Boyle MP, Bell S, Konstan M, McColley SA, Kang L, Patel N, et al. The investigational CFTR corrector, VX-809 (lumacaftor) co-administered with the oral potentiator ivacaftor improved CFTR and lung function in F509-8DEL homozygous patients: phase II study results. Pediatric Pulmonology 2012;47 Suppl 35:315. [ABSTRACT NO.: 260] [CENTRAL: 921644] [CFGD REGISTER: BD169b]
-
- Boyle MP, Bell S, Konstan MW, McColley SA, Wisseh S, Spencer-Green G. VX-809, an investigational CFTR corrector, in combination with VX-770, an investigational CFTR potentiator, in subjects with CF and homozygous for the F508DEL-CFTR Mutation. Pediatric Pulmonology 2011;46 Suppl 34:287. [ABSTRACT NO.: 212] [CENTRAL: 848840] [CFGD REGISTER: BD169a]
-
- Boyle MP, Bell SC, Konstan MW, McColley SA, Rowe SM, Rietschel E, et al. A CFTR corrector (lumacaftor) and a CFTR potentiator (ivacaftor) for treatment of patients with cystic fibrosis who have a phe508del CFTR mutation: A phase 2 randomised controlled trial. Lancet. Respiratory Medicine 2014;2(7):527-38. [CENTRAL: 994993] [CFGD REGISTER: BD169d] [EMBASE: 2014458184] - PubMed
-
- Boyle MP, Bell SC, Konstan MW, McColley SA, Rowe SM, Rietschel E, et al. Supplementary Appendix to "A CFTR corrector (lumacaftor) and a CFTR potentiator (ivacaftor) for treatment of patients with cystic fibrosis who have a phe508del CFTR mutation: A phase 2 randomised controlled trial.". Lancet. Respiratory Medicine 2014;2(7):527-38. Online. [CENTRAL: 997711] [CFGD REGISTER: BD169e] - PubMed
Clancy 2012 {published data only}
-
- Clancy JP, Rowe SM, Accurso FJ, Aitken ML, Amin RS, Ashlock MA, et al. Results of a phase IIa study of VX-809, an investigational CFTR corrector compound, in subjects with cystic fibrosis homozygous for the F508del-CFTR mutation. Thorax 2012;67(1):12-8. [CENTRAL: 806692] [CFGD REGISTER: BD166c] - PMC - PubMed
-
- Clancy JP, Rowe SM, Accurso FJ, Ballmann M, Boyle MP, DeBoeck C, et al. A phase II, randomized, placebo-controlled, clinical trial of four doses of VX-809 in CF patients homozygous for the F508del CFTR mutation. Pediatric Pulmonology 2010;45 Suppl 33(S33):298. [ABSTRACT NO.: 224] [CENTRAL: 848845] [CFGD REGISTER: BD166b]
-
- Clancy JP, Rowe SM, Liu B, Hathorne H, Dong Q, Wisseh S, et al. Variability of nasal potential difference measurements in clinical testing of CFTR modulators. Pediatric Pulmonology 2011;46 Suppl 34(S34):283. [ABSTRACT NO.: 202] [CENTRAL: 848842] [CFGD REGISTER: BD166d // BD165n]
-
- Clancy JP, Spencer-Green G, for theVX-809-101SG. Clinical evaluation of VX-809, a novel investigational oral F508del-CFTR corrector, in subjects with cystic fibrosis homozygous for the F508del-CFTR mutation. Journal of Cystic Fibrosis 2010;9 Suppl 1:S20. [ABSTRACT NO.: 73] [CENTRAL: 848846] [CFGD REGISTER: BD166a]
Davies 2018a {published data only}
-
- Davies JC, Moskowitz SM, Brown C, Horsley A, Mall MA, McKone EF, et al. VX-659-tezacaftor-ivacaftor in patients with cystic fibrosis and one or two Phe508del alleles. New England Journal of Medicine 2018;379(17):1599-611. [CENTRAL: CN-01650323] [CFGD REGISTER: BD260] [EMBASE: 624591628] [PMID: ] - PMC - PubMed
Davies 2018b {published data only}
-
- Colombo C, Tullis E, Davies JC, McKee C, DeSouza C, Waltz D, et al. Preliminary safety and efficacy of triple combination CFTR modulator regimens in CF. Italian Journal of Pediatrics 2018;44(Suppl 1):6. [ABSTRACT NO.: 03] [CFGD REGISTER: BD248b]
-
- Davies JC, Colombo C, Tullis E, Mckee C, Desouza C, Waltz D, et al. Preliminary safety and efficacy of triple combination CFTR modulator regimens in cystic fibrosis. Journal of Cystic Fibrosis 2018;17(Suppl 3):S3. [CENTRAL: CN-01730786] [CFGD REGISTER: BD248a] [EMBASE: 622930757]
-
- Davies JC, Moskowitz SM, Brown C, Horsley A, Mall MA, McKone EF, et al. VX-659-tezacaftor-ivacaftor in patients with cystic fibrosis and one or two Phe508del alleles. New England Journal of Medicine 2018;379(17):1599-611. [CENTRAL: CN-01650323] [CFGD REGISTER: BD260] [DOI: 10.1056/NEJMoa1807119] [EMBASE: 624591628] [PMID: 30334693 ] - DOI - PMC - PubMed
-
- Tullis E, Colombo C, Davies J, Wark P, McKee C, Desouza C, et al. Preliminary safety and efficacy of triple-combination CFTR modulator regimens. Respirology 2018;23(Suppl 1):33. [ABSTRACT NO.: TO 026] [CFGD REGISTER: BD248c]
Donaldson 2014 {published data only}
-
- Donaldson SH, Shoemaker S, Mandagere A, Troha J. Novel modifiers of CFTR: emerging clinical experience with GSNOR inhibitors. Pediatric Pulmonology 2014;49 Suppl 38:154. [ABSTRACT NO.: S10.2] [CENTRAL: 1015872] [CFGD REGISTER: BD217b]
-
- Donaldson SH, Taylor-Cousar JL, Rosenbluth D, Zeitlin P, Chmiel J, Jain M, et al. Safety, tolerability, and pharmacokinetics of the intravenous S-nitrosoglutathione reductase inhibitor N6022: an ascending-dose study in subjects homozygous for the F508DEL-CFTR mutation. Pediatric Pulmonology 2014;49 Suppl 38:308. [ABSTRACT NO.: 258] [CENTRAL: 1012386] [CFGD REGISTER: BD217a]
-
- NCT01746784. Safety and Pharmacokinetic Study of N6022 in Subjects With Cystic Fibrosis Homozygous for the F508del CFTR Mutation (SNO1) [A Phase 1b, randomized, double-blind, placebo-controlled, dose escalation study of N6022 to evaluate safety and pharmacokinetics in subjects with cystic fibrosis homozygous for the F508del-CFTR mutation (SNO1)]. clinicaltrials.gov/ct2/show/NCT01746784 (first posted 11 December 2012). [CLINICALTRIALS.GOV: NCT01746784]
Donaldson 2017 {published data only}
-
- Donaldson SH, Solomon GM, Zeitlin PL, Flume PA, Casey A, McCoy K, et al. Pharmacokinetics and safety of cavosonstat (N91115) in healthy and cystic fibrosis adults homozygous for F508DEL-CFTR. Journal of Cystic Fibrosis 2017;16(3):371-379. Online supplementary tables and figures. [CFGD REGISTER: BD226c] - PubMed
-
- Donaldson SH, Solomon GM, Zeitlin PL, Flume PA, Casey A, McCoy K, et al. Pharmacokinetics and safety of cavosonstat (N91115) in healthy and cystic fibrosis adults homozygous for F508DEL-CFTR. Journal of Cystic Fibrosis 2017;16(3):371-9. [CFGD REGISTER: BD226b] - PubMed
-
- Donaldson SH. Safety and pharmacokinetics of N91115 in patients with cystic fibrosis homozygous for the F508DEL-CFTR mutation. Pediatric Pulmonology 2015;50 Suppl 41:293. [ABSTRACT NO.: 270] [CENTRAL: 1092200] [CFGD REGISTER: BD226a]
-
- NCT02275936. Study of N91115 in patients with cystic fibrosis homozygous F508del-CFTR mutation (SNO4) [A phase 1b, randomized, double-blind, placebo-controlled, parallel, group study of N91115 to evaluate safety and pharmacokinetics in patients with cystic fibrosis homozygous for the F508del-CFTR mutation]. clinicaltrials.gov/ct2/show/NCT02275936 (first posted 27 October 2014).
Donaldson 2018 {published data only}
-
- Donaldson S, Pilewski J, Griese M, Dong Q, Lee PS, for theVX11-661-101SG. VX-661, an investigational CFTR corrector, in combination with ivacaftor, a CFTR potentiator, in patients with CF and homozygous for the F508Del-CFTR mutation: interim analysis. Journal of Cystic Fibrosis 2013;12 Suppl 1:S14. [ABSTRACT NO.: WS7.3] [CENTRAL: 872941] [CFGD REGISTER: BD190a]
-
- Donaldson SH, Pilewski JM, Cooke J, Himes-Lekstrom J, VX11-661-101 SG. Addition of VX-661, an investigational CFTR corrector, to ivacaftor, a CFTR potentiator, in patients with CF and heterozygous for F508DEL/G551D-CFTR. Pediatric Pulmonology 2014;49 Suppl 38:308-9. [ABSTRACT NO.: 260] [CENTRAL: 1012385] [CFGD REGISTER: BD190c]
-
- Donaldson SH, Pilewski JM, Griese M, Cooke J, Viswanathan L, Tullis E, et al. Tezacaftor/ivacaftor in subjects with cystic fibrosis and F508del/F508del-CFTR or F508del/G551D-CFTR. American Journal of Respiratory and Critical Care Medicine 2018;197(2):214-224. Online data supplement. [CFGD REGISTER: BD190f] - PMC - PubMed
-
- EUCTR2011-003821-93-DE. A phase 2, multicenter, double blinded, placebo controlled study to evaluate safety, efficacy, pharmacokinetics, and pharmacodynamics of VX-661 monotherapy and vx-661/ivacaftor cotherapy in subjects with cystic fibrosis, homozygous or heterozygous for the f508del CFTR mutation. www.who.int/trialsearch/Trial2.aspx?TrialID=EUCTR2011-003821-93-DE (first received 2011). [CENTRAL: CN-01882341] [CFGD REGISTER: BD190g]
Heijerman 2019 {published data only}
-
- Department of Error. Erratum: Department of Error (The Lancet (2019) 394(10212) (1940–1948), (S0140673619325978), (10.1016/S0140-6736(19)32597-8)). Lancet 2020;395(10238):1694. [CENTRAL: CN-02164017] [CFGD REGISTER: BD268c] [EMBASE: 2006013175] [PMID: ] - PubMed
-
- Heijerman H, McKone E, Downey DG, Mall M, Ramsey B, Rowe S, et al. Phase 3 efficacy and safety of the ELX/TEZ/ iva triple combination in people with CF homozygous for the F508del mutation. Pediatric Pulmonology 2019;54 Suppl 2:347. [CENTRAL: CN-01990652] [CFGD REGISTER: BD268a] [EMBASE: 629389111]
-
- Heijerman HGM, McKone EF, Downey DG, Van Braeckel E, Rowe SM, Tullis E, et al. Efficacy and safety of the elexacaftor plus tezacaftor plus ivacaftor combination regimen in people with cystic fibrosis homozygous for the F508del mutation: a double-blind, randomised, phase 3 trial. Lancet 2019;394(10212):1940-8. [CENTRAL: CN-02006814] [CFGD REGISTER: BD268b] [DOI: 10.1016/S0140-6736(19)32597-8] [EMBASE: 2003873327] [PMID: ] - DOI - PMC - PubMed
-
- NCT03525548. A study of VX-445 combination therapy in CF subjects homozygous for F508del (F/F). clinicaltrials.gov/ct2/show/NCT03525548 (first posted 15 May 2018). [EUDRACT NUMBER: 2018-000184-89]
Horsley 2017 {published and unpublished data}
-
- Horsley A, Burr L, Kotsimbos T, Ledson M, Schwarz C, Simmonds N, et al. Safety, pharmacokinetics and pharmacodynamics of the CFTR corrector FDL169. Journal of Cystic Fibrosis 2018;17(Suppl 3):S42. [CFGD REGISTER: BD250a]
-
- Horsley AR, Blaas S, Burr L, Caroll M, Downey DG, Drevinek P, et al. Novel CFTR corrector FDL169: safety, pharmacokinetics and pharmacodynamics. Journal of Cystic Fibrosis 2018;17 Suppl 3:S42. [ABSTRACT NO.: EPS3.06] [CFGD REGISTER: BD250b]
Keating 2018 {published data only}2017‐000797‐11
-
- Keating D, Marigowda G, Burr L, Daines C, Mall MA, McKone EF, et al. VX-445-Tezacaftor-Ivacaftor in Patients with Cystic Fibrosis and One or Two Phe508del Alleles. New England Journal of Medicine 2018;379(17):1612-20. [CENTRAL: CN-01650324] [CFGD REGISTER: BD259] [EMBASE: 624591484] [PMID: ] - PMC - PubMed
-
- NCT03227471. A study of VX-445 in healthy subjects and subjects with cystic fibrosis [A phase 1/2 study of VX-445 in healthy subjects and subjects with cystic fibrosis]. clinicaltrials.gov/ct2/show/NCT03227471 (first posted 24 July 2017).
McCarty 2002 {published data only}
-
- Ahrens RC, Standaert TA, Launspach J, Han SH, Teresi ME, Aitken ML, et al. Use of nasal potential difference and sweat chloride as outcome measures in multicenter clinical trials in subjects with cystic fibrosis. Pediatric Pulmonology 2002;33(2):142-50. [CENTRAL: 385693] [CFGD REGISTER: BD136d ] - PubMed
-
- Aitken ML, Ahrens RC, Karlin DA, Konstan MW, McNamara SC, Regelman WE, et al. Safety of a phase I double-blind placebo-controlled dose escalation trial of oral CPX in adult CF patients. Pediatric Pulmonology 1998;26 Suppl 17:276. [CENTRAL: 385694] [CFGD REGISTER: BD136b]
-
- McCarty NA, Standaert TA, Teresi M, Tuthill C, Launspach J, Kelley TJ, et al. A phase I randomized, multicenter trial of CPX in adult subjects with mild cystic fibrosis. Pediatric Pulmonology 2002;33(2):90-8. [CENTRAL: 377220] [CFGD REGISTER: BD136c] [PMID: ] - PubMed
-
- McCarty NA, Weatherly MR, Kelley TJ, Konstan MW, Milgram LJ, Teresi M, et al. Multicenter phase I trial of CPX in adults patients with mild CF: results of nasal potential difference measurements. Pediatric Pulmonology 1998;26 Suppl 17:276. [CENTRAL: 291449] [CFGD REGISTER: BD136a]
Middleton 2019 {published data only}
-
- Fajac I, Van Brunt K, Daines C, Durieu I, Goralski J, Heijerman H, et al. Impact of elexacaftor/tezacaftor/ivacaftor triple combination therapy on health-related quality of life in people with cystic fibrosis heterozygous for F508del and a minimal function mutation: results from a Phase 3 clinical study. Journal of Cystic Fibrosis 2020;19:S118-9. [CENTRAL: CN-02140149] [CFGD REGISTER: BD267c] [EMBASE: 2006056615]
-
- Jain R, Mall M, Drevinek P, Lands L, McKone E, Polineni D, et al. Phase 3 efficacy and safety of the ELX/TEZ/ iva triple combination in people with CF and F508del/minimal function genotypes. Pediatric Pulmonology 2019;54 Suppl:346-7. [CENTRAL: CN-01987255] [CFGD REGISTER: BD267a] [EMBASE: 629389084]
-
- Middleton PG, Mall MA, Drevinek P, Lands LC, McKone EF, Polineni D, et al. Elexacaftor-tezacaftor-ivacaftor for cystic fibrosis with a single phe508del allele. New England Journal of Medicine 2019;381(19):1809-19. [CENTRAL: CN-02004607] [CFGD REGISTER: BD267b] [DOI: 10.1056/NEJMoa1908639] [PMID: ] - DOI - PMC - PubMed
-
- NCT03525444. A phase 3 study of VX-445 combination therapy in subjects with cystic fibrosis heterozygous for the f508del mutation and a minimal function mutation (F/MF) [A phase 3, randomized, double-blind, controlled study evaluating the efficacy and safety of VX-445 combination therapy in subjects with cystic fibrosis who are heterozygous for the f508del mutation and a minimal function mutation (F/MF)]. clinicaltrials.gov/show/NCT03525444 (first received 15 May 2018). [CENTRAL: CN-01659552] [CFGD REGISTER: BD267d] [EUDRACT NUMBER: 2018-000183-28]
PROGRESS 2017 {published data only}
-
- Konstan M, McKone E, Moss R, Marigowda G, Cooke J, Lubarsky B, et al. Evidence of reduction in annual rate of FEV1 decline and sustained benefits with lumacaftor and ivacaftor (LUM/IVA) in patients (pts) with cf homozygous for F508DEL-CFTR. Pediatric Pulmonology 2016;51 Suppl 45:260. [ABSTRACT NO.: 180] [CFGD REGISTER: BD213p // BD214p]
-
- Konstan MW, McKone EF, Moss RB, Marigowda G, Tian S, Waltz D, et al. Assessment of safety and efficacy of long-term treatment with combination lumacaftor and ivacaftor therapy in patients with cystic fibrosis homozygous for the F508del-CFTR mutation (PROGRESS): a phase 3, extension study. Lancet. Respiratory Medicine 2017;5(2):107-118. Online supplementary appendix. [CFGD REGISTER: BD213r // BD214r] - PubMed
-
- Konstan MW, McKone EF, Moss RB, Marigowda G, Tian S, Waltz D, et al. Assessment of safety and efficacy of long-term treatment with combination lumacaftor and ivacaftor therapy in patients with cystic fibrosis homozygous for the F508del-CFTR mutation (PROGRESS): a phase 3, extension study. Lancet. Respiratory Medicine 2017;5(2):107-18. [CFGD REGISTER: BD213q // BD214q] [PMID: ] - PubMed
-
- NCT01931839. A phase 3 rollover study of lumacaftor in combination with ivacaftor in subjects 12 years and older with cystic fibrosis [A phase 3, rollover study to evaluate the safety and efficacy of long-term treatment with lumacaftor in combination with ivacaftor in subjects aged 12 Years and older with cystic fibrosis, homozygous or heterozygous for the F508del-CFTR mutation]. clinicaltrials.gov/ct2/show/NCT01931839 (first posted 29 August 2013). [CLINICALTRIALS.GOV: NCT01931839]
Ratjen 2017 {published data only}
-
- Anonymous. Corrections [Corrections: efficacy and safety of lumacaftor and ivacaftor in patients aged 6-11 years with cystic fibrosis homozygous for F508del-CFTR: a randomised, placebo-controlled phase 3 trial (The Lancet Respiratory Medicine (2017) 5(7) (557-567)(S2213260017302151)(10.1016/S2213-2600(17)30215-1))]. Lancet Respiratory Medicine 2017 Aug;5(8):e28. [CENTRAL: CN-01473292] [CFGD REGISTER: BD233k] [EMBASE: 617478198] [PMID: ] - PubMed
-
- Brody A, Nagle SK, Owen C, Marigowda G, Waltz D, Goldin J, et al. Effect of lumacaftor/ivacaftor on total, bronchiectasis, and air trapping computed tomography scores in children homozygous for F508DEL-CFTR: exploratory imaging substudy. Pediatric Pulmonology 2017;52 Suppl 47:286. [CFGD REGISTER: BD233d]
-
- Brody AS, Nagle S, Hug C, Marigowda G, Waltz D, Goldin J, et al. Effect of lumacaftor/ivacaftor on total, bronchiectasis, and air trapping computed tomography (CT) scores in children homozygous for F508del-CFTR: exploratory imaging substudy. Thorax 2017;72(Supplement 3):A57. [CENTRAL: CN-01643820] [CFGD REGISTER: BD233e] [EMBASE: 619739057]
-
- Brody AS, Nagle S, Hug C, Marigowda G, Waltz D, Goldin J, et al. Effect of lumacaftor/ivacaftor on total, bronchiectasis and air trapping computed tomography (CT) scores in children homozygous for F508del-CFTR: exploratory imaging substudy. Thorax 2017;72(Suppl 3):A57. [CFGD REGISTER: BD233e]
-
- Milla C, Ratjen F, Marigowda G, Liu F, Waltz D, Rosenfeld M. Safety, tolerability, and pharmacodynamics of combination lumacaftor/ivacaftor therapy in patients aged 6-11 yrs with CF homozygous for the F508DEL-CFTR mutation. Pediatric Pulmonology 2016;51 Suppl:259. [CENTRAL: CN-01212610] [CFGD REGISTER: BD233j] [EMBASE: 612358598]
Rubenstein 1998 {published data only}
-
- Rubenstein RC, Zeitlin PL. A pilot clinical trial of oral sodium 4-phenylbutyrate (Buphenyl) in deltaF508-homozygous cystic fibrosis patients: partial restoration of nasal epithelial CFTR function. American Journal of Respiratory and Critical Care Medicine 1998;157(2):484-90. [CENTRAL: 201485] [CFGD REGISTER: BD146b] [EMBASE: 1998064104] [PMID: ] - PubMed
-
- Rubenstein RC, Zeitlin PL. A randomized, double blind, placebo-controlled trial of sodium 4-phenylbutyrate (Buphenyl) in deltaF508-homozygous cystic fibrosis patients: partial restoration of nasal epithelial CFTR function. Pediatric Pulmonology 1997;Suppl 14:272. [CENTRAL: 291563] [CFGD REGISTER: BD146a] - PubMed
Taylor‐Cousar 2017 {published data only}
-
- Flume P, Lekstrom-Himes J, Fischer Biner R, Simard C, Downey DG, Zhou H, et al. A phase 3, open-label study of tezacaftor/ivacaftor (TEZ/IVA) therapy, interim analysis of pooled safety, and efficacy in patients homozygous for F508del-CFTR. Journal of Cystic Fibrosis 2018;17 Suppl 3:S64-5. [CFGD REGISTER: BD236d]
-
- Ingenito E, Nair N, Yi B, Lekstrom-Himes J, Elborn JS, Rowe SM. Retrospective analysis of physiological response patterns to tezacaftor/ivacaftor in patients with cystic fibrosis homozygous for F508DEL-CFTR or heterozygous for F508DEL-CFTR and a residual function mutation. Thorax 2018;73(Suppl 4):A42-3. [CENTRAL: CN-02002310] [CFGD REGISTER: BD236i // BD237h] [EMBASE: 627697348]
-
- Smith D, Flume P, Lekstrom-Himes J, Fischer Biner R, Simard C, Downey D, et al. Phase 3 interim analysis: tezacaftor/ivacaftor (TEZ/IVA) in patients homozygous for F508delcystic fibrosis transmembrane conductance regulator (CFTR). Respirology 2019;24(S1):30. [ABSTRACT NO.: TO017] [CENTRAL: CN-02002181] [CFGD REGISTER: BD236j] [EMBASE: 626940397]
-
- Sommerburg O, Yang Y, Rizio AA, Loop B, You X, Kosinski M, et al. Effects of tezacaftor/ivacaftor (TEZ/IVA) treatment in patients with cystic fibrosis and F508del/F508del-CFTR: patient-reported outcomes in a Phase 3, randomised, controlled trial (EVOLVE). Pneumologie 2019;73(Suppl 1). [CENTRAL: CN-01960604] [CFGD REGISTER: BD236h] [EMBASE: 628475389]
-
- Sutharsan S, Taylor-Cousar J, Lekstrom-Himes J, Wang L, Lu Y, Elborn JS. Efficacy and safety of tezacaftor/ivacaftor in patients aged >= 12 years with CF homozygous for F508del-CFTR: a randomized placebo (PBO)-controlled phase 3 trial. Pneumologie (Stuttgart, Germany) 2018;72(Suppl 1):S36. [CFGD REGISTER: BD236e]
TRAFFIC 2015 {published data only}
-
- Anstead M, Tupayachi G, Murphy D, Autry E, Bulkley V, Kuhn R. Lumacaftor/ivacaftor: real world experience in a CF center. Pediatric Pulmonology 2016;51 Suppl:302. [CFGD REGISTER: BD213s // BD214s]
-
- De Boeck C. Long-term clinical effects of CFTR co-therapy with lumacaftor/ivacaftor. Pediatric Pulmonology 2015;50:135-7. [CENTRAL: 1163954] [CFGD REGISTER: BD213m/BD214m] [EMBASE: 72081237] [SYMPOSIUM SUMMARY: S9.1]
-
- De Boeck K, Elborn J, Ramsey B, Boyle MP, Konstan MW, Huang X, et al. Efficacy and safety of lumacaftor+ivacaftor combination therapy in patients with CF homozygous for F508DEL-CFTR by FEV1 subgroups. Pediatric Pulmonology 2015;50 Suppl 41:283. [ABSTRACT NO.: 245] [CENTRAL: 1092180] [CFGD REGISTER: BD213f/BD214f]
-
- Elborn J, Wainwright CE, Ramsey B, Huang X, Margowda G, Waltz D, et al. Effect of lumacaftor in combination with ivacaftor in patients with cystic fibrosis who are homozygous for F508-DEL-CFTR: the TRAFFIC Study. Pediatric Pulmonology 2014;49 Suppl 38:304. [ABSTRACT NO.: 249] [CENTRAL: 1012382] [CFGD REGISTER: BD213a]
-
- Elborn JS, Ramsey B, Boyle MP, Wainwright C, Konstan M, Huang X, et al. Lumacaftor in combination with ivacaftor in patients with cystic fibrosis who are homozygous for the F508del-CFTR mutation. Journal of Cystic Fibrosis 2015;14 Suppl 1:S1. [ABSTRACT NO.: WS01.3] [CENTRAL: 1077209] [CFGD REGISTER: BD213e/BD214d]
TRANSPORT 2015 {published data only}
-
- Anstead M, Tupayachi G, Murphy D, Autry E, Bulkley V, Kuhn R. Lumacaftor/ivacaftor: real world experience in a CF center. Pediatric Pulmonology 2016;51 Suppl:302. [CFGD REGISTER: BD213s // BD214s]
-
- De Boeck C. Long-term clinical effects of CFTR co-therapy with Lumacaftor/Ivacaftor. Pediatric Pulmonology 2015;50:135-7. [CENTRAL: 1163954] [CFGD REGISTER: BD214m/BD213m] [EMBASE: 72081237] [SYMPOSIUM SUMMARY: S9.1]
-
- De Boeck K, Elborn J, Ramsey B, Boyle MP, Konstan MW, Huang X, et al. Efficacy and safety of lumacaftor+ivacaftor combination therapy in patients with CF homozygous for F508DEL-CFTR by FEV1 subgroups. Pediatric Pulmonology 2015;50 Suppl 41:283. [ABSTRACT NO.: 245] [CENTRAL: 1092180] [CFGD REGISTER: BD214f/BD213f]
-
- Elborn JS, Ramsey B, Boyle MP, Wainwright C, Konstan M, Huang X, et al. Lumacaftor in combination with ivacaftor in patients with cystic fibrosis who are homozygous for the F508del-CFTR mutation. Journal of Cystic Fibrosis 2015;14 Suppl 1:S1. [ABSTRACT NO.: WS01.3] [CENTRAL: 1077209] [CFDG REGISTER: BD214d/BD213e]
-
- Elborn JS, Ramsey BW, Boyle MP, Konstan MW, Huang X, Marigowda G, et al. Efficacy and safety of lumacaftor/ivacaftor combination therapy in patients with cystic fibrosis homozygous for Phe508del CFTR by pulmonary function subgroup: a pooled analysis. Lancet. Respiratory Medicine 2016;4(8):617-26. [CENTRAL: 1157425] [CFGD REGISTER: BD214i/BD213i] [DOI: 10.1016/S2213-2600(16)30121-7] [PMID: ] - DOI - PMC - PubMed
Zeitlin 2002 {published data only}
-
- Zeitlin PL, Diener-West M, Rubenstein RC, Boyle MP, Lee CK, Brass-Ernst L. Evidence of CFTR function in cystic fibrosis after systemic administration of 4-phenylbutyrate. Molecular Therapy 2002;6(1):119-26. [CENTRAL: 409030] [CFGD REGISTER: BD148] [PMID: ] - PubMed
References to studies excluded from this review
Berkers 2014 {published data only}
-
- Berkers G, Vijftigschild L, Bronsveld I, Arets H, Winter-de Groot K, Heijerman H, et al. A beta-2 agonist as a CFTR activator in CF; the ABBA study. Pediatric Pulmonology 2014;49 Suppl 38:299-300. [ABSTRACT NO.: 236] [CENTRAL: 1012380] [CFGD REGISTER: BD212]
Chadwick 1998 {published data only}
-
- Chadwick S, Browning JE, Stern M, Cheng SH, Gruenert DC, Geddes DM, et al. Nasal application of glycerol in DF508 cystic fibrosis patients. Pediatric Pulmonology 1998;Suppl 17:278. [ABSTRACT NO.: 275] [CENTRAL: 208568] [CFGD REGISTER: BD147]
Chilvers 2017 {published data only}
-
- Chilvers M, Davies JC, Ratjen F, Milla C, Owen CA, Tian S, et al. Long-term safety and efficacy of lumacaftor/ivacaftor therapy in patients aged 6-11 years with cystic fibrosis homozygous for the F508del-CFTR mutation (F/F). Journal of Cystic Fibrosis 2019;18 Suppl 1:S23. [ABSTRACT NO.: WS12-4] [CENTRAL: CN-02011205] [CFGD REGISTER: BD232c] [EMBASE: 2001976603]
-
- Chilvers M, Owen C, Marigowda G, Tian S, Solomon M, Black P, et al. Safety and efficacy of lumacaftor/ ivacaftor in patients aged =6 years with cf homozygous for F508DEL-CFTR (phase 3 extension study). Pediatric Pulmonology 2017;52 Suppl 47:319. [CFGD REGISTER: BD232b]
-
- Chilvers M, Tian S, Marigowda G, Bsharat M, Hug C, Solomon M, et al. An open-label extension (EXT) study of lumacaftor/ivacaftor (LIM/IVA) therapy in patients (pts) aged 6-11 years (yrs) with cystic fibrosis (CF) homozygous for F508del-CFTR. Journal of Cystic Fibrosis 2017;16 Suppl 1:S77. [ABSTRACT NO: 52] [CENTRAL: 1383248] [CFGD REGISTER: BD232a] [CLINICALTRIALS.GOV: NCT01897233]
-
- NCT01897233. Study of lumacaftor in combination with ivacaftor in subjects 6 through 11 years of age with cystic fibrosis, homozygous for the F508del-CFTR mutation [A phase 3, open-label study to evaluate the pharmacokinetics, safety, and tolerability of lumacaftor in combination with ivacaftor in subjects 6 through 11 years of age with cystic fibrosis, homozygous for the F508del-CFTR mutation]. clinicaltrials.gov/ct2/show/NCT01897233 (first posted 2013 July 11). [CFGD REGISTER: BD232d] [CLINICALTRIALS.GOV: NCT01897233]
Drevinek 2017 {published data only (unpublished sought but not used)}
-
- Drevinek P, Pready N, Lamontagne N, Montgomery S, Henig N. QR-010 via inhalation is safe, well tolerated and achieves systemic concentrations in a single ascending dose study in subjects with cystic fibrosis homozygous for the F508del CFTR mutation. Journal of Cystic Fibrosis 2017;16 Suppl 1:S73-4. [CFGD REGISTER: BD244a]
-
- Elborn S, Bouisset F, Checcio T, Perquin J, Lamontagne N, Montgomery S, et al. A first-in-human, phase 1b, dose escalation study of QR-010, a novel antisense oligonucleotide administered in subjects with cystic fibrosis homozygous for the F508del CFTR mutation. Paediatric Pulmonology 2017;52 Suppl 47:289. [CFGD REGISTER: BD244b]
Leonard 2012 {published data only}
-
- Leonard A, Dingemanse J, Lebecque P, Leal T. Oral miglustat in homozygous F508del CF patients. Journal of Cystic Fibrosis 2010;9 Suppl 1:S20. [ABSTRACT NO.: 75] [CENTRAL: 921950] [CFGD REGISTER: BD193a]
-
- Leonard A, Lebecque P, Dingemanse J, Leal T. A randomized placebo-controlled trial of miglustat in cystic fibrosis based on nasal potential difference. Journal of Cystic Fibrosis 2012;11:231-6. [CENTRAL: 840524] [CFGD REGISTER: BD193b] [PMID: ] - PubMed
NCT00945347 {published data only}
-
- NCT00945347. Does a nasal instillation of miglustat normalize the nasal potential difference in cystic fibrosis patients? [Does a nasal instillation of miglustat normalize the nasal potential difference in cystic fibrosis patients homozygous for the F508del mutation? A randomized, double blind placebo-controlled study]. clinicaltrials.gov/show/NCT00945347 (first posted 24 July 2009).
NCT01899105 {published data only}
-
- NCT01899105. A phase 1 study to investigate the food effect of lumacaftor in combination with ivacaftor [A phase 1, randomized, single-dose, open-label crossover study to investigate the effect of food on the relative bioavailability of 2 fixed-dose combinations of lumacaftor and ivacaftor tablet formulations in healthy adult subjects]. clinicaltrials.gov/show/NCT01899105 (first posted 15 July 2013). [CLINICALTRIALS.GOV: NCT01899105]
NCT03447262 {published data only}
-
- NCT03447262. A study evaluating the long term safety and efficacy of VX-659 combination therapy. clinicaltrials.gov/ct2/show/NCT03447262 (first posted 27 February 2018).
NCT03525574 {published data only}
-
- NCT03525574. A study evaluating the long-term safety and efficacy of VX-445 combination therapy. clinicaltrials.gov/ct2/show/NCT03525574 (first posted 15 May 2018).
NCT03537651 {published data only}
-
- NCT03537651. A study to evaluate the safety and efficacy of long-term treatment with TEZ/IVA in CF subjects with an F508del CFTR mutation. clinicaltrials.gov/ct2/show/NCT03537651 (first posted 25 May 2018).
NCT03601637 {published data only}
-
- NCT03601637. Safety and pharmacokinetic study of lumacaftor/ivacaftor in subjects 1 to less than 2 years of age with cystic fibrosis, homozygous for F508del. clinicaltrials.gov/ct2/show/NCT03601637 (first posted 26 July 2018).
NCT03633526 {published data only}
-
- NCT03633526. Evaluation of VX-659/TEZ/IVA in cystic fibrosis subjects 6 through 11 years of age. clinicaltrials.gov/ct2/show/NCT03633526 (first posted 16 August 2018).
NCT03691779 {published data only}
-
- NCT03691779. Evaluation of VX 445/TEZ/IVA in cystic fibrosis subjects 6 through 11 years of age. clinicaltrials.gov/ct2/show/NCT03691779 (first posted 02 October 2018).
NCT04043806 {published data only}
-
- NCT04043806. A study evaluating the long-term safety of VX-445 combination therapy. clinicaltrials.gov/ct2/show/NCT04043806 (first posted 02 August 2019).
NCT04058366 {published data only}
-
- NCT04058366. Study evaluating the long-term safety and efficacy of VX-445 combination therapy. clinicaltrials.gov/ct2/show/NCT04058366 (first posted 15 August 2019).
NCT04105972 {published data only}
-
- NCT04105972. A study evaluating the efficacy and safety of VX-445/tezacaftor/ivacaftor in cystic fibrosis subjects, homozygous for F508del. clinicaltrials.gov/ct2/show/NCT04105972 (first posted 26 September 2019).
NCT04183790 {published data only}
-
- NCT04183790. Evaluation of long-term safety and efficacy of VX-445 combination therapy in subjects with cystic fibrosis who are 6 years of age and older. clinicaltrials.gov/ct2/show/NCT04183790 (first posted 03 December 2019).
NCT04235140 {published data only}
-
- NCT04235140. Long-term safety of lumacaftor/ivacaftor in subjects with cystic fibrosis who are homozygous for F508del and 12 to <24 months of age at treatment initiation. clinicaltrials.gov/ct2/show/NCT04235140 (first posted 21 January 2020).
NCT04362761 {published data only}
-
- NCT04362761. A study evaluating the long-term safety of elexacaftor combination therapy. clinicaltrials.gov/ct2/show/NCT04362761 (first posted 27 April 2020).
NCT04537793 {published data only}
-
- NCT04537793. Evaluation of ELX/TEZ/IVA in fFibrosis (CF) subjects 2 through 5 Years. clinicaltrials.gov/ct2/show/NCT04537793 (first posted 03 September 2020).
NCT04545515 {published data only}
-
- NCT04545515. A study evaluating the long-term safety and efficacy of elexacaftor/tezacaftor/ivacaftor in cystic fibrosis (CF) subjects 6 years and older and F/MF genotypes. clinicaltrials.gov/ct2/show/NCT04545515 (first posted 11 September 2020).
Nick 2014 {published data only}
-
- Nick JA, Rodman D, St Clair C, Jones MC, Li H, Higgins M, et al. Effect of ivacaftor in patients with cystic fibrosis, residual CFTR function, and FEV1 ≥40% of predicted, N-of-1 study. Pediatric Pulmonology 2014;49 Suppl 38:285. [ABSTRACT NO.: 196] [CENTRAL: 1012379] [CFGD REGISTER: BD211a ]
-
- Nick JA, Rodman D, St Clair C, Jones MC, Li H, Higgins M. Utilization of an "n-of-1" study design to test the effect of ivacaftor in CF patients with residual CFTR function and FEV1 >40% of predicted. Pediatric Pulmonology 2014;49:188-9. [CENTRAL: 1008991] [CFGD REGISTER: BD211b] [EMBASE: 71616032]
Rowe 2017 {published data only}
-
- Chuang C, Rizio A, Loop B, Lekstrom-Himes J, You X, Kosinski M, et al. Effects of tezacaftor/ivacaftor treatment in patients heterozygous for f508del-cftr and a residual function mutation: patient reported outcomes in a phase 3 randomized, controlled trial. Paediatric Pulmonology 2018;53 Suppl 2:S264. [CFGD REGISTER: BD237e] [CTG: ] [DOI: 10.1002/ppul.24152] - DOI
-
- Chuang C-C, Rizio AA, Loop B, Lekstrom-Himes J, You X, Kosinski M, et al. Effects of tezacaftor/ivacaftor (TEZ/IVA) treatment in patients heterozygous for F508DEL-CFTR and a residual function mutation: patient-reported outcomes in a phase 3 randomized, controlled trial (expand). Thorax 2018;73:A41. [CENTRAL: CN-01934562] [CFGD REGISTER: BD237f] [EMBASE: 627697165]
-
- Fischer R, Rizio AA, Loop B, Lekstrom-Himes J, You X, Kosinski M, et al. Effects of tezacaftor/ivacaftor (TEZ/IVA) treatment in patients heterozygous for F508del-CFTR and a residual function mutation: patient-reported outcomes in a Phase 3, randomised, controlled trial (EXPAND). Pneumologie 2019;73(Suppl 1). [CENTRAL: CN-01960601] [CFGD REGISTER: BD237g] [EMBASE: 628475378]
-
- Fischer R, Rowe SM, Davies JC, Nair N, Han L, Lekstrom-Himes J. Efficacy and safety of tezacaftor/ivacaftor in patients (Pts) aged >= 12 Years with CF heterozygous for F508del and a residual function mutation: a randomized, double-blind, placebo-controlled, crossover phase 3 study. Pneumologie 2018;72 Suppl 1:S35. [CFGD REGISTER: BD237d] [DOI: 10.1055/s-0037-1619210] [NCT: 02392234] - DOI
-
- Ingenito E, Nair N, Yi B, Lekstrom-Himes J, Elborn JS, Rowe SM. Retrospective analysis of physiological response patterns to tezacaftor/ivacaftor in patients with cystic fibrosis homozygous for F508DEL-CFTR or heterozygous for F508DEL-CFTR and a residual function mutation. Thorax 2018;73(Suppl 4):A42-3. [CFGD REGISTER: BD237h] [DOI: 10.1136/thorax-2018-212555.75] - DOI
Rubenstein 2006 {published data only}
-
- Rubenstein RC, Propert KJ, Reenstra WW, Skotleski ML. A pilot trial of the combination of phenylbutyrate and genistein. Pediatric Pulmonology 2006;41 Suppl 29:294. [ABSTRACT NO.: 248] [CENTRAL: 593141] [CFGD REGISTER: BD149]
Sumner 2014 {published data only}
-
- Sumner Jones SG, Alton EW, Boyd A, Chang SH, Davies JC, Davies LA, et al. Molecular analyses of vector delivery and gene expression in a multidose trial of non-viral gene therapy in patients with CF. Pediatric Pulmonology 2014;49 Suppl 38:302. [ABSTRACT NO.: 243] [CENTRAL: 1012381] [CFGD REGISTER: BD210b]
-
- Waller MD, Harman KM, Boyd A, Chang SH, Gill DR, Griesenbach U, et al. Measurement of CFTR function in cystic fibrosis patients in response to multidose CFTR gene therapy. Pediatric Pulmonology 2014;49 Suppl 38:249. [ABSTRACT NO.: 97] [CENTRAL: 1012378] [CFGD REGISTER: BD210a]
Ziady 2015 {published data only}
-
- Ziady AG, Lin S, Heltshe SL, Kelley T, Muhlebach MS, Accurso FJ, et al. Protein expression in CF primary airway epithelia following treatment with VX-809 reveals significant changes in pkc-mediated signalling, proton and iron transport, and lipid metabolism. Pediatric Pulmonology 2015;50 Suppl 41:300. [ABSTRACT NO.: 290] [CENTRAL: 1092203] [CFGD REGISTER: BD225]
References to studies awaiting assessment
Downey 2019 {published data only}
-
- Downey D, Flume P, Jain M, Fajac I, Schwarz C, Pressler T, et al. Initial results evaluating combinations of the novel CFTR corrector PTI-801, potentiator PTI-808, and amplifier PTI-428 in cystic fibrosis subjects. Journal of Cystic Fibrosis 2019;18 Suppl 1:S10. [CENTRAL: CN-01990618] [CFGD REGISTER: BD269a] [EMBASE: 2001976571]
-
- Flume P, Downey DG, Jain M, Fajac I, Schwarz C, Pressler T, et al. Evaluation of novel CFTR modulator combinations of the corrector PTI-801, potentiator PTI-808, and amplifier PTI-428 in CF subjects. Pediatric Pulmonology 2019;54 Suppl 2:348. [CENTRAL: CN-01989480] [CFGD REGISTER: BD269c] [EMBASE: 629387551]
-
- Jain M, Pilewski J, Flume P, Taylor-Cousar J, Rowe S, Milla C, et al. Initial results evaluating the add-on effect of the novel CFTR corrector PTI-801 in cystic fibrosis subjects. Journal of Cystic Fibrosis 2019;18 Suppl 1:S10-1. [CENTRAL: CN-02007011] [CFGD REGISTER: BD269b] [EMBASE: 2001976532]
EudraCT 2019‐000750‐63 {published data only}
-
- EudraCT 2019-000750-63. A phase 2 study of ABBV-3067 alone and in combination with ABBV-2222 in cystic fibrosis subjects who are homozygous for the F508del mutation. www.clinicaltrialsregister.eu/ctr-search/search?query=2019-000750-63 (first posted 31 October 2019).
Hunt 2017 {published data only}
-
- Hunt K, St Clair C, Curran-Everett D, Solomon GM, Saavedra MT, Nick JA, et al. CFTR effects of oral sildenafil in combination with lumacaftor/ivacaftor in adults with CF. Pediatric Pulmonology 2017;52(Suppl 47):322. [CFGD REGISTER: IB117]
Munck 2020 {published data only}
-
- Munck A, Kerem E, Ellemunter H, Campbell D, Wang LT, Ahluwalia N, et al. Tezacaftor/ivacaftor in people with cystic fibrosis heterozygous for minimal function CFTR mutations. Journal of Cystic Fibrosis 2020 Jun 13 [epub ahead of print];S1569-1993(20):30128-4. [CENTRAL: CN-02142331] [CFGD REGISTER: BD274b] [DOI: 10.1016/j.jcf.2020.04.015] [EMBASE: 2006729203] [PMID: ] - DOI - PubMed
-
- NCT02516410. A study to evaluate the efficacy and safety of VX-661 in combination with ivacaftor in subjects aged 12 years and older with cystic fibrosis, heterozygous for the F508del-CFTR mutation. clinicaltrials.gov/ct2/show/NCT02516410 first posted 05 August 2015. [CFGD REGISTER: BD274a]
NCT02951195 {published data only}
-
- NCT02951195. A study evaluating the safety of VX-152 combination therapy in adults with cystic fibrosis [A phase 2, randomized, double blind, controlled study to evaluate the safety of VX-152 combination therapy in adults with cystic fibrosis]. clinicaltrials.gov/ct2/show/NCT02951195 (first posted 01 November 2016).
NCT03447249 {published data only}
-
- NCT03447249. A phase 3, randomized, double-blind, controlled study evaluating the efficacy and safety of VX-659 combination therapy in subjects with cystic fibrosis who are heterozygous for the F508del mutation and a minimal function mutation (F/MF). clinicaltrials.gov/ct2/show/NCT03447249 (first posted 27 February 2018). [EUDRACT NUMBER: 2017-004132-11]
NCT03460990 {published data only}
-
- NCT03460990. A study of VX-659 combination therapy in CF subjects homozygous for F508del (F/F). clinicaltrials.gov/ct2/show/NCT03460990 (first posted 09 March 2018). [EUDRACT NUMBER: 2017-004133-82]
NCT03768089 {published data only}
-
- EudraCT 2018-000126-55. A phase 1/2 Study of VX-121 in healthy subjects and in subjects with cystic fibrosis. www.clinicaltrialsregister.eu/ctr-search/search?query=2018-000126-55 (first posted 15 March 2018).
-
- NCT03768089. Study of VX-121 in healthy subjects and in subjects with cystic fibrosis. clinicaltrials.gov/ct2/show/NCT03768089 (first posted 07 December 2018). [2018-000126-55 ( EudraCT Number )]
NCT03911713 {published data only}
-
- NCT03911713. A phase 2 study to evaluate efficacy and safety of VX-561 in subjects aged 18 years and older with cystic fibrosis. clinicaltrials.gov/ct2/show/NCT03911713 (first posted 11 April 2019). [EUDRACT NUMBER: 2018-003970-28]
NCT03912233 {published data only}
-
- EUCTR2018-002496-18-PT. A study to evaluate the safety and efficacy of VX-121 combination therapy in subjects with cystic fibrosis [A phase 2, randomized, double-blind, controlled study to evaluate the safety and efficacy of VX-121 combination therapy in subjects aged 18 years and older with cystic fibrosis]. www.who.int/trialsearch/Trial2.aspx?TrialID=EUCTR2018-002496-18-PT (first received 2019). [CENTRAL: CN-02068097] [CFGD REGISTER: BD277b]
-
- NCT03912233. A study to evaluate the safety and efficacy of VX-121 combination therapy in subjects with cystic fibrosis [A phase 2, randomized, double-blind, controlled study to evaluate the safety and efficacy of VX-121 combination therapy in subjects aged 18 years and older with cystic fibrosis]. clinicaltrials.gov/show/NCT03912233 (first received 11 April 2019). [CENTRAL: CN-01912167] [CFGD REGISTER: BD277a]
NCT04058353 {published data only}
-
- NCT04058353. A phase 3 study of VX-445 combination therapy in cystic fibrosis (CF) subjects heterozygous for F508del and a gating or residual function mutation (F/G and F/RF genotypes). clinicaltrials.gov/ct2/show/NCT04058353 (first posted 15 August 2019). [EUDRACT NUMBER: 2018-002835-76]
NCT04353817 {published data only}
-
- NCT04353817. A study evaluating efficacy and safety of elexacaftor/tezacaftor/ivacaftor in subjects 6 through 11 years of age with cystic fibrosis and F/MF genotypes. clinicaltrials.gov/ct2/show/NCT04353817 (first posted 20 April 2020). [EUDRACT NUMBER: 2019-003554-86]
PELICAN {published data only}
-
- EUCTR2017-002181-42-DE. GLPG2737 on top of Orkambi in subjects with cystic fibrosis [A Phase IIa, randomized, double-blind, placebo-controlled study to evaluate GLPG2737 in Orkambi-treated subjects with cystic fibrosis homozygous for the F508del mutation]. www.who.int/trialsearch/Trial2.aspx?TrialID=EUCTR2017-002181-42-DE (first received 2017). [CENTRAL: CN-01887243] [CFGD REGISTER: BD272b]
-
- NCT03474042. GLPG2737 on top of orkambi in subjects with cystic fibrosis [A phase iia, randomized, double-blind, placebo-controlled study to evaluate GLPG2737 in orkambi-treated subjects with cystic fibrosis homozygous for the f508del mutation]. clinicaltrials.gov/show/NCT03474042 (first received 2018 March 22). [CFGD REGISTER: BD272a]
-
- Koningsbruggen-Rietschel S, Conrath K, Fischer R, Sutharsan S, Kempa A, Gleiber W, et al. GLPG2737 in lumacaftor/ivacaftor-treated CF subjects homozygous for the F508del mutation: a randomized phase 2A trial (PELICAN). Journal of Cystic Fibrosis 2020;19(2):292-8. [CENTRAL: CN-01999311] [CFGD REGISTER: BD272c] [EMBASE: 2003281625] [PMID: ] - PubMed
Rio‐CF {published data only (unpublished sought but not used)}
-
- Derichs N, Taylor-Cousar J, Tullis E, Davies J, Nazareth D, Downey DG, et al. Safety, tolerability and early signs of efficacy with riociguat for the treatment of adult phe508del homozygous cystic fibrosis patients: study design and rationale for the Rio-CF study. Journal of Cystic Fibrosis 2017;16 Suppl 1:S36. [CFGD REGISTER: BD246b]
-
- NCT02170025. Early signs of efficacy study with riociguat in adult homozygous delta F508 cystic fibrosis patients [Multi-center phase 2 study to assess the safety, tolerability and early signs of efficacy of tid orally administered BAY63-2521 in adult delta F508 homozygous cystic fibrosis patients]. clinicaltrials.gov/ct2/show/results/NCT02170025 (first posted 23 June 2014).
-
- Taylor-Cousar JL, Tullis E, Derichs N, Davies JC, Nazareth D, Downey R, et al. Riociguat for the treatment of adult phe508del homozygous cystic fibrosis: efficacy data from the phase II Rio-CF study. Journal of Cystic Fibrosis 2018;17 Suppl 3:S67. [CFGD REGISTER: BD246a] - PubMed
Taylor‐Cousar 2019 {published data only}
-
- Taylor-Cousar J, Gifford AH, Flume P, Sawicki GS, Pilewski JM, Jain M, et al. Initial results evaluating the first-in-class CFTR amplifier, PTI-428, in subjects with CF on background treatment with tezacaftor/ ivacaftor. Pediatric Pulmonology 2019;54 Suppl 2:332. [CENTRAL: CN-01988388] [CFGD REGISTER: BD270] [EMBASE: 629388001]
Wainwright 2019 {published data only}
-
- Wainwright C, Stick S, Goldin J, Lekstrom-Himes J, Wang L, Campbell D, et al. Change in low-dose chest computed tomography (CT) scores after 72 weeks of tezacaftor/ivacaftor (TEZ/IVA) in patients (pts) with cystic fibrosis and ppFEV1 >=70%: an exploratory phase 2 study. Journal of Cystic Fibrosis 2019;18 Suppl 1:S11-2. [CENTRAL: CN-02009338] [CFGD REGISTER: BD275] [EMBASE: 2001976227]
References to ongoing studies
ALBATROSS {published data only (unpublished sought but not used)}BD247
-
- Bell S, De Boeck K, Drevinek P, Plant B, Barry P, Elborn S, et al. GLPG2222 in subjects with cystic fibrosis and the F508del/Class III mutation on stable treatment with ivacaftor: results from a phase II study (ALBATROSS). Journal of Cystic Fibrosis 2018;17 Suppl 3:S2. [ABSTRACT NO.: WS01.4] [CFGD REGISTER: BD247a]
-
- Bell S, De Boeck K, Drevinek P, Plant B, Barry P, Elborn S, et al. Results from a phase II study- ALBATROSS - evaluation of GLPG2222 in subjects with CF and the F508del/class III mutation on stable treatment with ivacaftor. Pediatric Pulmonology 2018;53 Suppl 2:249. [ABSTRACT NO.: 269] [CFGD REGISTER: BD247b]
-
- Bell SC, Barry PJ, De Boeck K, Drevinek P, Elborn JS, Plant BJ, et al. CFTR activity is enhanced by the novel corrector GLPG2222, given with and without ivacaftor in two randomized trials. Journal of Cystic Fibrosis 2019;18(5):700-7. [CENTRAL: CN-01936893] [CFGD REGISTER: BD247c // BD254c] [DOI: 10.1016/j.jcf.2019.04.014] [EMBASE: 2001903987] [PMID: ] - DOI - PubMed
-
- NCT03045523. A study to evaluate GLPG2222 in ivacaftor-treated subjects with cystic fibrosis. clinicaltrials.gov/ct2/show/NCT03045523 (first posted 07 February 2017). [STUDY NO.: GLPG2222-CL-201]
FLAMINGO {published data only (unpublished sought but not used)}
-
- NCT03119649. A study to evaluate multiple doses of GLPG2222 in adult subjects with cystic fibrosis. clinicaltrials.gov/ct2/show/NCT03119649 (first posted 18 April 2017). [STUDY NO.: GLPG2222-CL-202]
-
- Ent KC, Minic P, Verhulst S, Van Brackel E, Flume P, Boas S, et al. GLPG2222 in subjects with cystic fibrosis homozygous for F508del: results from a phase II study (FLAMINGO). Journal of Cystic Fibrosis 2018;17 Suppl 3:S42. [ABSTRACT NO.: EPS3.05 ] [CFGD REGISTER: BD254a]
-
- Ent KC, Minic P, Verhulst S, Van Brackel E, Flume P, Boas S, et al. GLPG2222 in subjects with cystic fibrosis homozygous for F508del: results from a phase II study (FLAMINGO). Pediatric Pulmonology 2018;53 Suppl 2:250. [ABSTRACT NO.: 271] [CFGD REGISTER: BD254b]
Jain 2018 {published data only (unpublished sought but not used)}
-
- Jain M, Flume P, Escobar H, Taylor-Cousar JL, Pressler T, Liou TG, et al. Initial results evaluating third generation CFTR corrector PTI-801 in CF subjects. Paediatric Pulmonology 2018;53 Suppl 2:246. [CFGD REGISTER: BD257]
Meijer 2016 {published data only}
-
- Meijer L, Hery-Arnaud G, Le Berre R, Nowak E, Le Roux L, Gueganton L, et al. Rosco-CF, a safety and efficacy clinical trial of (R)-roscovitine in CF patients. Journal of Cystic Fibrosis 2016;15 Suppl 1:S42. [ABSTRACT NO.: ePS03.7] [CENTRAL: 1157464] [CFGD REGISTER: BD230a]
-
- Meijer L, Hery-Arnaud G, Le Berre R, Nowak E, Le Roux L, Gueganton L, et al. ROSCO-CF, a safety and efficacy clinical trial of (r)-roscovitine in CF patients. Pediatric Pulmonology 2016;51 Suppl 45:269. [CFGD REGISTER: BD230b]
-
- Meijer L, Hery-Arnaud G, Le Berre R, Nowak E, Rault G, Mottier D. ROSCO-CF, a safety and efficacy clinical trial of (R)-roscovitine in cystic fibrosis patients. Journal of Cystic Fibrosis 2018;17 Suppl 3:S25. [CFGD REGISTER: BD230c]
-
- NCT02649751. Evaluation of (R)-roscovitine safety and effects in subjects with cystic fibrosis, homozygous for the F508del-CFTR mutation (ROSCO-CF) [A phase II, dose ranging, multicenter, double-blind, placebo controlled study to evaluate safety and effects of (R)-Roscovitine in adults subjects with cystic fibrosis, carrying 2 cystic fibrosis causing mutations with at least one F508del-CFTR mutation and chronically infected with Pseudomonas aeruginosa, a study involving 36 CF patients (24 treated, 12 controls). ROSCO-CF]. clinicaltrials.gov/ct2/show/NCT02649751 (first posted 07 January 2016).
NCT02070744 {published data only}
-
- NCT02070744. Study to evaluate safety and efficacy of VX-661 in combination with ivacaftor in subjects with cystic fibrosis, homozygous for the F508del-CFTR mutation with an open-label expansion [A phase 2, randomized, multicenter, double blind, placebo controlled study to evaluate safety, efficacy, pharmacokinetics, and pharmacodynamics of VX-661 in combination with ivacaftor for 12 weeks in subjects with cystic fibrosis, homozygous for the F508del CFTR mutation with an open-label extension]. clinicaltrials.gov/ct2/show/NCT02070744 (first posted 25 February 2014). [CLINICALTRIALS.GOV: NCT02070744]
NCT02323100 {published data only}
-
- NCT02323100. Glycerol phenylbutyrate corrector therapy for CF (Cystic Fibrosis) (GPBA) [A double blind, placebo controlled, dose escalation trial of glycerol phenylbutyrate corrector therapy for cystic fibrosis]. clinicaltrials.gov/ct2/show/NCT02323100 (first posted 23 December 2014).
NCT02412111 {published data only}
-
- NCT02412111. A phase 3 study of VX-661 in combination with ivacaftor in subjects aged 12 years and older with cystic fibrosis, who have one F508del-CFTR mutation and a second mutation that has been demonstrated to be clinically responsive to ivacaftor [A phase 3, randomized, double-blind, Ivacaftor-controlled, parallel-group study to evaluate the efficacy and safety of VX-661 in combination with ivacaftor in subjects aged 12 years and older with cystic fibrosis, heterozygous for the F508del-CFTR mutation and a second CFTR allele with a gating defect that Is clinically demonstrated to be ivacaftor responsive]. clinicaltrials.gov/ct2/show/NCT02412111 (first posted 08 April 2015).
NCT02589236 {published data only}
-
- NCT02589236. Study of cavosonstat (N91115) in patients with CF homozygous for the F508del-CFTR mutation (SNO-6) [A phase 2, randomized, double-blind, placebo-controlled, parallel-group study of N91115 to evaluate efficacy and safety in patients with cystic fibrosis who are homozygous for the F508del-CFTR mutation treated with lumacaftor/ivacaftor]. clinicaltrials.gov/ct2/show/NCT02589236 (first posted 28 October 2015).
NCT02718495 {published data only}
-
- NCT02718495. Study assessing PTI-428 safety, tolerability, and pharmacokinetics in subjects with cystic fibrosis [A phase I/II, multi-center, randomized, placebo-controlled, study designed to assess the safety, tolerability, and pharmacokinetics of PTI-428 in subjects with cystic fibrosis]. clinicaltrials.gov/ct2/show/NCT02718495 (first posted 24 March 2016).
NCT02730208 {published data only}
-
- NCT02730208. A study to evaluate the effect of VX-661 in combination with ivacaftor on chest imaging endpoints in subjects with cystic fibrosis, homozygous for the F508del CFTR mutation [A phase 2, randomized, placebo-controlled, double-blind study to evaluate the effect of VX-661 in combination with ivacaftor on chest imaging endpoints in subjects aged 12 years and older with cystic fibrosis, homozygous for the F508del CFTR mutation]. clinicaltrials.gov/ct2/show/NCT02730208 (first posted 06 April 2016).
NCT03258424 {published data only}
-
- NCT03258424. Study assessing PTI-428 safety, tolerability, and pharmacokinetics in subjects with cystic fibrosis on KALYDECO® as background therapy [A phase I, randomized, placebo-controlled, study designed to assess the safety, tolerability, and pharmacokinetics of PTI-428 in subjects with cystic fibrosis]. clinicaltrials.gov/ct2/show/NCT03258424 (first posted 23 August 2017).
NCT03559062 {published data only}
-
- NCT03559062. A study to evaluate efficacy and safety of tez/iva in subjects aged 6 through 11 years with cystic fibrosis [A phase 3, double-blind, parallel-group study to evaluate the efficacy and safety of tezacaftor in combination with ivacaftor in subjects aged 6 through 11 years with cystic fibrosis, homozygous or heterozygous for the F508del-CFTR mutation]. clinicaltrials.gov/ct2/show/NCT03559062 (first posted 15 June 2018).
NCT03625466 {published data only}
-
- EUCTR2017-003761-99-DE. A study of the effects of lumacaftor/ivacaftor on disease progression in subjects aged 2 through 5 years with cystic fibrosis, homozygous for f508del [An exploratory phase 2, 2-part, randomized, double blind, placebo controlled study with a long term, open label period to explore the impact of lumacaftor/ivacaftor on disease progression in subjects aged 2 through 5 years with cystic fibrosis, homozygous for f508del]. www.who.int/trialsearch/Trial2.aspx?TrialID=EUCTR2017-003761-99-DE (first received 2018). [CENTRAL: CN-01908852] [CFGD REGISTER: BD276b]
-
- NCT03625466. A study to explore the impact of lumacaftor/ivacaftor on disease progression in subjects aged 2 through 5 years with cystic fibrosis, homozygous for f508del [An exploratory phase 2, 2-part, randomized, double-blind, placebo-controlled study with a long-term, open-label period to explore the impact of lumacaftor/ivacaftor on disease progression in subjects aged 2 through 5 years with cystic fibrosis, homozygous for f508del]. clinicaltrials.gov/show/NCT03625466 (first received 10 August 2018). [CENTRAL: CN-01626171] [CFGD REGISTER: BD276a]
Schwarz 2020 {published data only}
-
- NCT03150719. A study to evaluate safety, efficacy, and tolerability of TEZ/IVA in Orkambi® (lumacaftor/ivacaftor) - experienced subjects with cystic fibrosis (CF) [Phase 3b, randomized, double-blind, placebo-controlled, parallel group study to assess the safety, efficacy, and tolerability of tezacaftor/ivacaftor (TEZ/IVA) in an Orkambi-experienced population who are homozygous for the F508del CFTR mutation]. clinicaltrials.gov/ct2/show/NCT03150719 (first posted 12 May 2017). [CFGD REGISTER: BD273a]
-
- Schwarz C, Sutharsan S, Epaud R, Klingsberg R, Fischer R, Rowe SM, et al. Safety, efficacy, and tolerability of tezacaftor/ivacaftor in cystic fibrosis patients who previously discontinued lumacaftor/ivacaftor due to respiratory adverse events: a randomized, double-blind, placebo-controlled phase 3b study. Pneumologie 2019;73(Suppl 1). [CENTRAL: CN-01960602] [CFGD REGISTER: BD273b] [EMBASE: 628475379]
-
- Schwarz C, Sutharsan S, Epaud R, Klingsberg RC, Fischer R, Rowe SM, et al. Tezacaftor/ivacaftor in people with cystic fibrosis who stopped lumacaftor/ivacaftor due to respiratory adverse events. Journal of Cystic Fibrosis 2020 Jun 23 [epub ahead of print];S1569-1993(20):30730-X. [CENTRAL: CN-02143375] [CFGD REGISTER: BD273c] [DOI: 10.1016/j.jcf.2020.06.001] [EMBASE: 2006829285] [PMID: ] - DOI - PMC - PubMed
Additional references
Amaral 2007
-
- Amaral MD, Kunzelmann K. Molecular targeting of CFTR as a therapeutic approach to cystic fibrosis. Trends in Pharmacological Sciences 2007;28(7):334-41. - PubMed
Aslam 2017
Bobadilla 2002
-
- Bobadilla JL, Macek M, Fine JP, Farrell PM. Cystic fibrosis: a worldwide analysis of CFTR mutations - correlation with incidence data and application to screening. Human Mutation 2002;19(6):575-606. - PubMed
CFMD 2013
-
- Cystic Fibrosis Centre at the Hospital for Sick Children in Toronto, Canada. Cystic fibrosis mutation database. www.genet.sickkids.on.ca/app (accessed 23 September 2013).
Colledge 1995
-
- Colledge WH, Abella BS, Southern KW, Ratcliff R, Jiang C, Cheng SH, et al. Generation and characterization of a delta F508 cystic fibrosis mouse model. Nature Genetics 1995;10(4):445-52. - PubMed
Deeks 2011
-
- Deeks JJ, Higgins JP, Altman DG. Chapter 9: Analysing data and undertaking meta-analysis. In: Higgins JP, Green S, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from handbook.cochrane.org.
EMA 2012
-
- European Medicines Agency. Report of the workshop on endpoints for cystic fibrosis clinical trials (EMA/769571/2012); November 2012. Available at www.ema.europa.eu/docs/en_GB/document_library/Report/2012/12/WC500136159....
Higgins 2003
Higgins 2011a
-
- Higgins JP, Altman DG, editor(s). Chapter 8: Assessing risk of bias in included studies. In: Higgins JP, Green S, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from handbook.cochrane.org.
Higgins 2011b
-
- Higgins JP, Deeks JJ, Altman DG on behalf of the CSMG . Chapter 16: Special topics in statistics. In: Higgins JP, Green S, editor(s). Cochrane Handbook of Systematic Reviews of Interventions. Version 5.1 (updated March 2011). The Cochrane Collaboration, 2011. Available from handbook.cochrane.org.
NICE 2016
-
- Lumacaftor–ivacaftor for treating cystic fibrosis homozygous for the F508del mutation. www.nice.org.uk/guidance/ta398 (accessed 01 September 2020).
Parmar 1998
-
- Parmar MK, Torri V, Stewart L. Extracting summary statistics to perform meta-analyses of the published literature for survival endpoints. Statistics in Medicine 1998;17:2815-34. - PubMed
Quittner 2009
-
- Quittner AL, Modi AC, Wainwright C, Otto K, Kirihara J, Montgomery AB. Determination of the minimal clinically important difference scores for the Cystic Fibrosis Questionnaire-Revised respiratory symptom scale in two populations of patients with cystic fibrosis and chronic Pseudomonas aeruginosa airway infection. Chest 2009;135(6):1610-8. - PMC - PubMed
Ramsey 2011
Riordan 1989
-
- Riordan JR, Rommens JM, Kerem BS, Alon N, Rozmahel R, Grzelczak Z, et al. Identification of the cystic fibrosis gene – cloning and characterization of complementary. Science 1989;245(4922):1066-72. - PubMed
Rogan 2011
Rowntree 2003
-
- Rowntree RK, Harris A. The phenotypic consequences of CFTR mutations. Annals of Human Genetics 2003;67(5):471-85. - PubMed
Rubenstein 1997
Skilton 2019
Southern 1997
Southern 2007
-
- Southern KW. Cystic fibrosis and formes frustes of CFTR-related disease. Respiration: International Review of Thoracic Diseases 2007;74(3):241-51. - PubMed
Van Goor 2011
-
- Van Goor F, Hadida S, Grootenhuis PD, Burton B, Stack JH, Straley KS, et al. Correction of the F508del-CFTR protein processing defect in vitro by the investigational drug VX-809. Proceedings of the National Academy of Sciences of the United States of America 2011;108(46):18843-8. [DOI: 10.1073/pnas.1105787108] - DOI - PMC - PubMed
Williamson 2002
-
- Williamson PR, Tudur Smith C, Hutton JL, Marson AG. Aggregate data meta-analysis with time-to-event outcomes. Statistics in Medicine 2002;21(11):3337-51. - PubMed
Wu 2018
-
- Wu HX, Zhu M, Xiong XF, Wei J, Zhuo KQ, Cheng DY. Efficacy and safety of CFTR corrector and potentiator combination therapy in patients with cystic fibrosis for the F508del-CFTR homozygous mutation: a systematic review and meta-analysis. Advances in Therapy 2018;36(2):451-61. [DOI: 10.1007/s12325-018-0860-4] [PMID: ] - DOI - PubMed
References to other published versions of this review
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical