

Post-acute COVID-19 associated with evidence of bystander T-cell activation and a recurring antibiotic-resistant bacterial pneumonia
- PMID: 33331820
- PMCID: PMC7775105
- DOI: 10.7554/eLife.63430
Post-acute COVID-19 associated with evidence of bystander T-cell activation and a recurring antibiotic-resistant bacterial pneumonia
Abstract
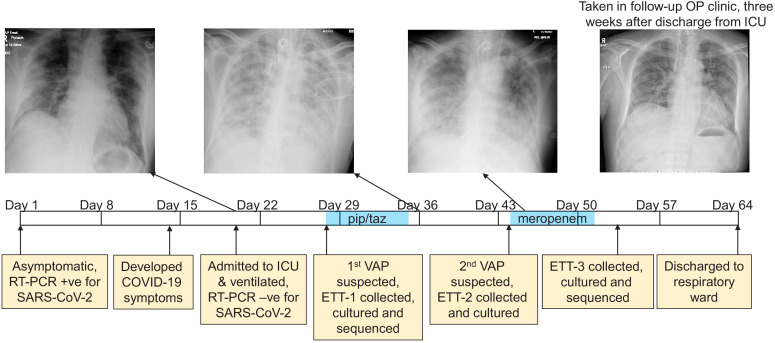
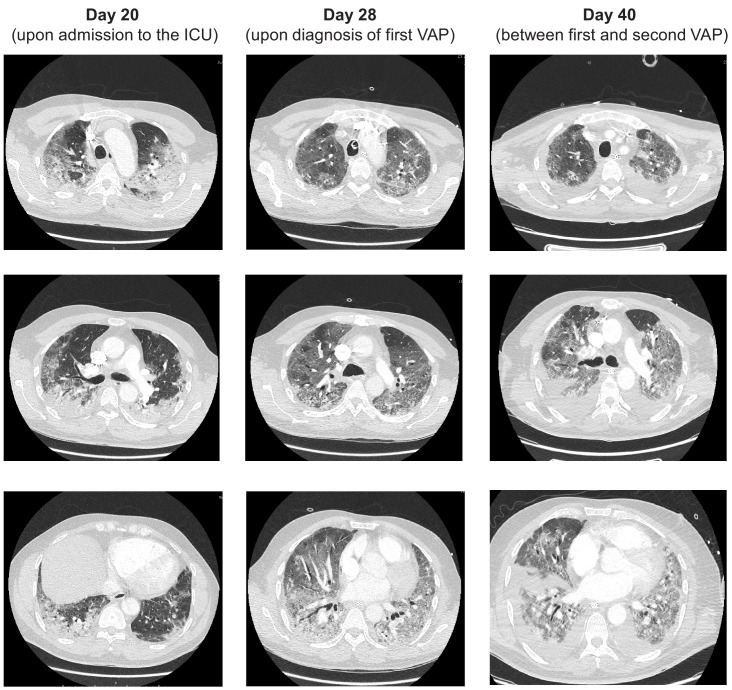
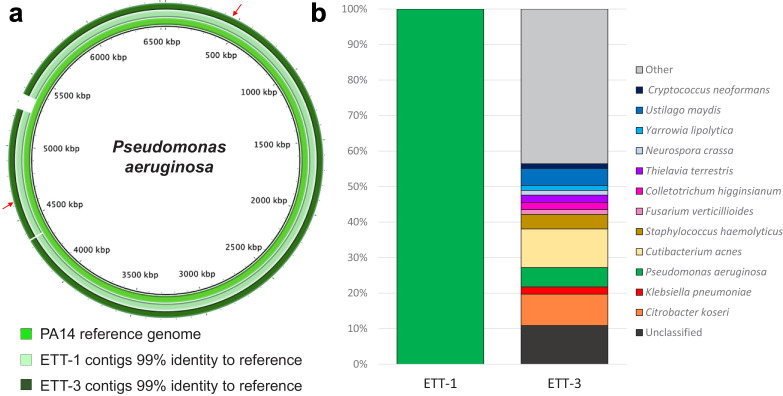
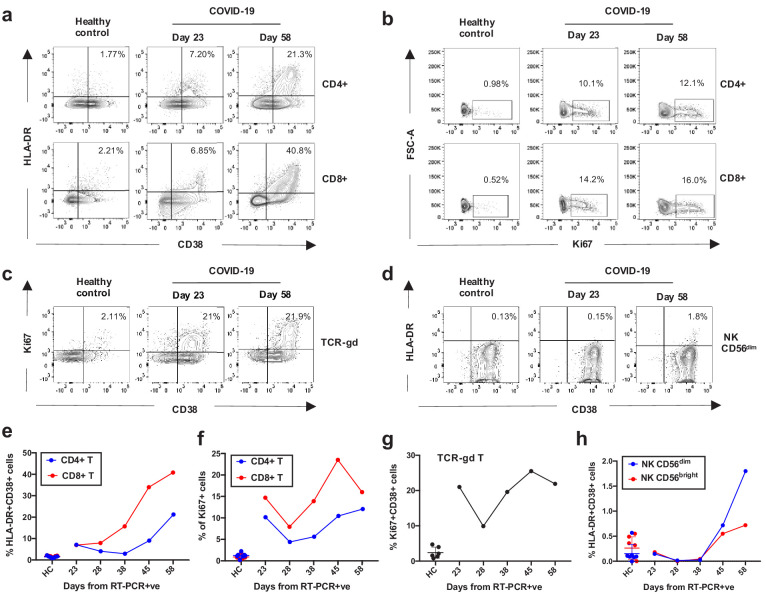
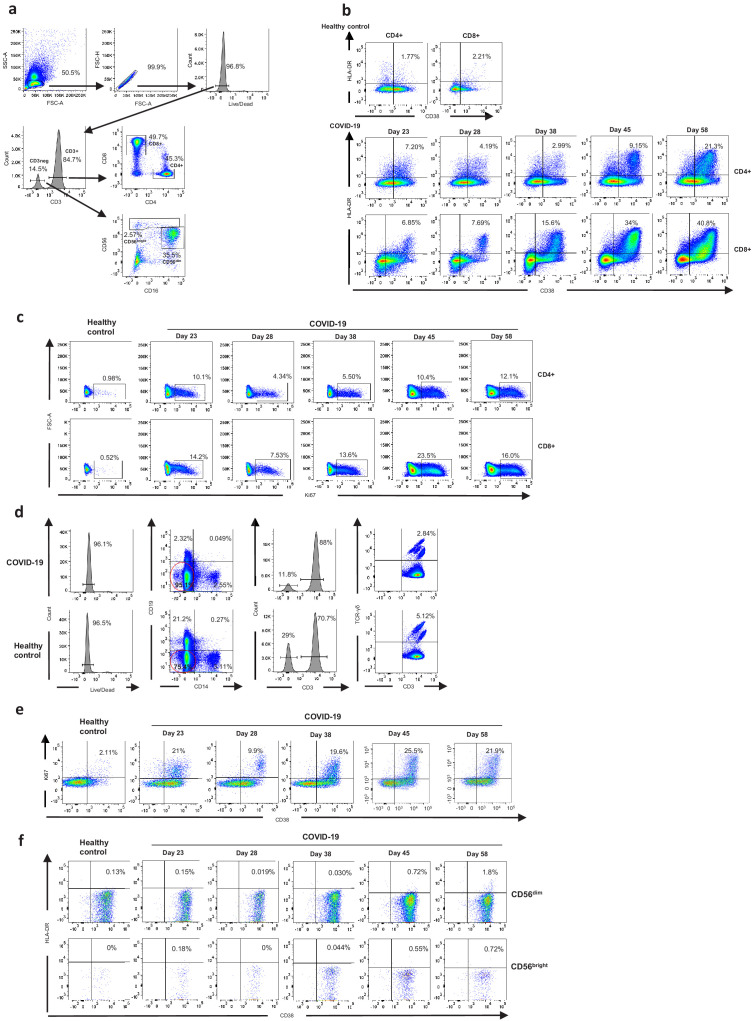
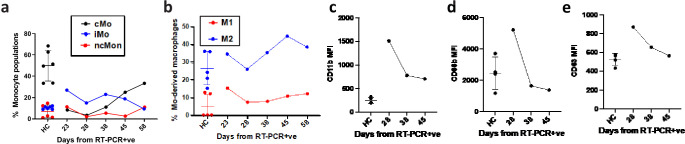
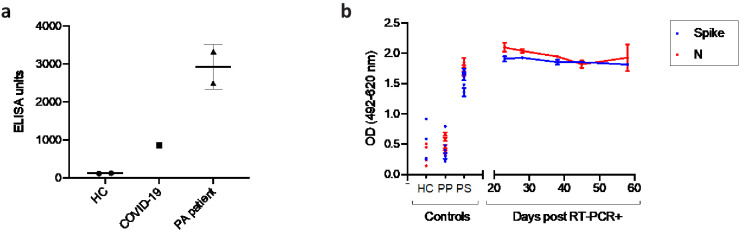
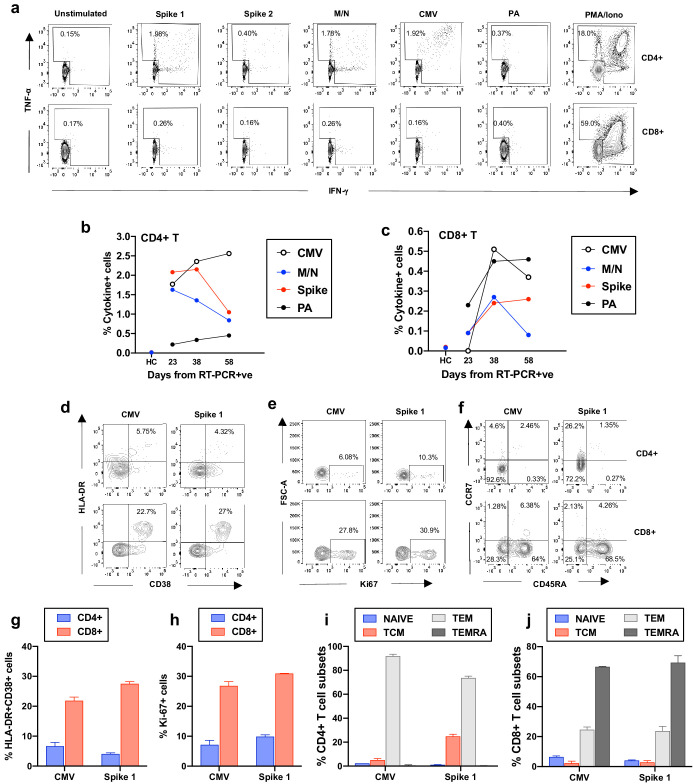
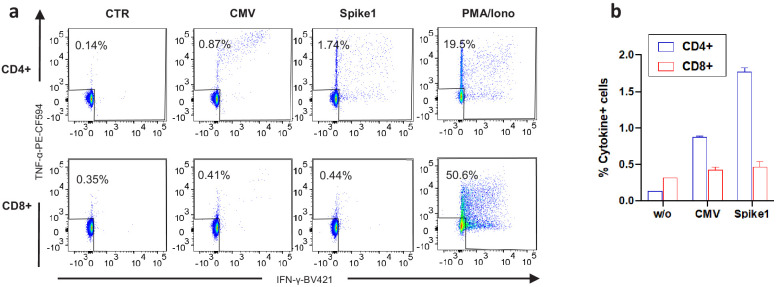
Here, we describe the case of a COVID-19 patient who developed recurring ventilator-associated pneumonia caused by Pseudomonas aeruginosa that acquired increasing levels of antimicrobial resistance (AMR) in response to treatment. Metagenomic analysis revealed the AMR genotype, while immunological analysis revealed massive and escalating levels of T-cell activation. These were both SARS-CoV-2 and P. aeruginosa specific, and bystander activated, which may have contributed to this patient's persistent symptoms and radiological changes.
Keywords: Pseudomonas aeruginosa; SARS-CoV-2; human; infectious disease; metagenomics; microbiology; t-cells activation.
© 2020, Gregorova et al.
Conflict of interest statement
MG, DM, TB, JS, FH, MA, DA, MT, AH, HB, CR, MA, AD, MS, EO, AG, AF, LW, BA, RB, DA, DB, CM, JS, SN, CC, NL, MC, LR, RM No competing interests declared
Figures
References
-
- Amanat F, Stadlbauer D, Strohmeier S, Nguyen THO, Chromikova V, McMahon M, Jiang K, Arunkumar GA, Jurczyszak D, Polanco J, Bermudez-Gonzalez M, Kleiner G, Aydillo T, Miorin L, Fierer DS, Lugo LA, Kojic EM, Stoever J, Liu STH, Cunningham-Rundles C, Felgner PL, Moran T, García-Sastre A, Caplivski D, Cheng AC, Kedzierska K, Vapalahti O, Hepojoki JM, Simon V, Krammer F. A serological assay to detect SARS-CoV-2 seroconversion in humans. Nature Medicine. 2020;26:1033–1036. doi: 10.1038/s41591-020-0913-5. - DOI - PMC - PubMed
-
- Arnold DT, Hamilton FW, Milne A, Morley AJ, Viner J, Attwood M, Noel A, Gunning S, Hatrick J, Hamilton S, Elvers KT, Hyams C, Bibby A, Moran E, Adamali HI, Dodd JW, Maskell NA, Barratt SL. Patient outcomes after hospitalisation with COVID-19 and implications for follow-up: results from a prospective UK cohort. medRxiv. 2020 doi: 10.1101/2020.08.12.20173526. - DOI - PMC - PubMed
-
- COVID-19 (Coronavirus Disease) Interim clinical guidance for management of patients with confirmed coronavirus disease (COVID-19) [November 4, 2020];2020 https://www.cdc.gov/coronavirus/2019-ncov/hcp/clinical-guidance-manageme...
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
