

Early Outcomes From Early Tracheostomy for Patients With COVID-19
- PMID: 33331855
- PMCID: PMC7747038
- DOI: 10.1001/jamaoto.2020.4837
Early Outcomes From Early Tracheostomy for Patients With COVID-19
Abstract
Importance: Decision-making in the timing of tracheostomy in patients with coronavirus disease 2019 (COVID-19) has centered on the intersection of long-standing debates on the benefits of early vs late tracheostomy, assumptions about timelines of infectivity of the novel coronavirus, and concern over risk to surgeons performing tracheostomy. Multiple consensus guidelines recommend avoiding or delaying tracheostomy, without evidence to indicate anticipated improvement in outcomes as a result.
Objective: To assess outcomes from early tracheostomy in the airway management of patients with COVID-19 requiring mechanical ventilation.
Design, setting, and participants: A retrospective medical record review was completed of 148 patients with reverse transcriptase-polymerase chain reaction-confirmed COVID-19 requiring mechanical ventilation at a single tertiary-care medical center in New York City from March 1 to May 7, 2020.
Interventions: Open or percutaneous tracheostomy.
Main outcomes and measures: The primary outcomes were time from symptom onset to (1) endotracheal intubation, (2) tracheostomy; time from endotracheal intubation to tracheostomy; time from tracheostomy to (1) tracheostomy tube downsizing, (2) decannulation; total time on mechanical ventilation; and total length of stay.
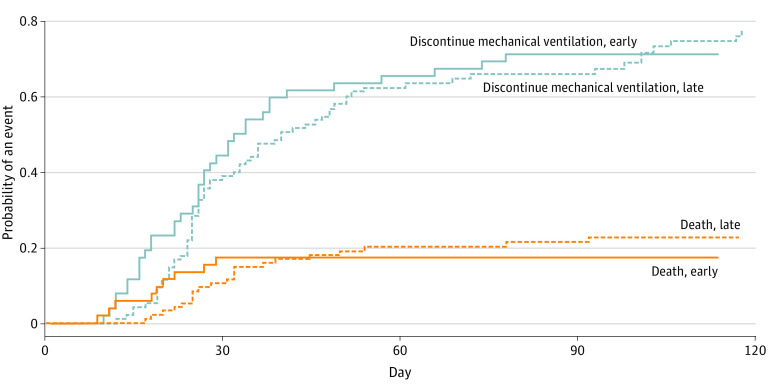
Results: Participants included 148 patients, 120 men and 28 women, with an overall mean (SD) age of 58.1 (15.8) years. Mean (SD; median) time from symptom onset to intubation was 10.57 (6.58; 9) days; from symptom onset to tracheostomy, 22.76 (8.84; 21) days; and from endotracheal intubation to tracheostomy, 12.23 (6.82; 12) days. The mean (SD; median) time to discontinuation of mechanical ventilation was 33.49 (18.82; 27) days; from tracheostomy to first downsize, 23.02 (13.76; 19) days; and from tracheostomy to decannulation, 30.16 (16.00; 26) days. The mean (SD; median) length of stay for all patients was 51.29 (23.66; 45) days. Timing of tracheostomy was significantly associated with length of stay: median length of stay was 40 days in those who underwent early tracheostomy (within 10 days of endotracheal intubation) and 49 days in those who underwent late tracheostomy (median difference, -8; 95% CI, -15 to -1). In a competing risks model with death as the competing risk, the late tracheostomy group was 16% less likely to discontinue mechanical ventilation (hazard ratio, 0.84; 95% CI, 0.55 to 1.28).
Conclusions and relevance: This cohort study from the first 2 months of the pandemic in New York City provides an opportunity to reconsider guidelines for tracheostomy for patients with COVID-19. Findings demonstrated noninferiority of early tracheostomy and challenges recommendations to categorically delay or avoid tracheostomy in this patient population. When aligned with emerging evidence about the timeline of infectivity of the novel coronavirus, this approach may optimize outcomes from tracheostomy while keeping clinicians safe.
Conflict of interest statement
Figures

Comment in
-
Shared Decision-making and Stakeholder Engagement in COVID-19 Tracheostomy.JAMA Otolaryngol Head Neck Surg. 2021 Jun 1;147(6):576-577. doi: 10.1001/jamaoto.2021.0184. JAMA Otolaryngol Head Neck Surg. 2021. PMID: 33764371 No abstract available.
-
Shared Decision-making and Stakeholder Engagement in COVID-19 Tracheostomy.JAMA Otolaryngol Head Neck Surg. 2021 Jun 1;147(6):576. doi: 10.1001/jamaoto.2021.0181. JAMA Otolaryngol Head Neck Surg. 2021. PMID: 33764373 No abstract available.
-
Shared Decision-making and Stakeholder Engagement in COVID-19 Tracheostomy.JAMA Otolaryngol Head Neck Surg. 2021 Jun 1;147(6):575-576. doi: 10.1001/jamaoto.2021.0178. JAMA Otolaryngol Head Neck Surg. 2021. PMID: 33764380 No abstract available.
References
-
- Michetti CP, Burlew CC, Bulger EM, Davis KA, Spain DA; Critical Care and Acute Care Surgery Committees of the American Association for the Surgery of Trauma . Performing tracheostomy during the Covid-19 pandemic: guidance and recommendations from the Critical Care and Acute Care Surgery Committees of the American Association for the Surgery of Trauma. Trauma Surg Acute Care Open. 2020;5(1):e000482. doi:10.1136/tsaco-2020-000482 - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
