

Intraoperative Oxygen Concentration and Neurocognition after Cardiac Surgery
- PMID: 33331902
- PMCID: PMC7855826
- DOI: 10.1097/ALN.0000000000003650
Intraoperative Oxygen Concentration and Neurocognition after Cardiac Surgery
Abstract
Background: Despite evidence suggesting detrimental effects of perioperative hyperoxia, hyperoxygenation remains commonplace in cardiac surgery. Hyperoxygenation may increase oxidative damage and neuronal injury leading to potential differences in postoperative neurocognition. Therefore, this study tested the primary hypothesis that intraoperative normoxia, as compared to hyperoxia, reduces postoperative cognitive dysfunction in older patients having cardiac surgery.
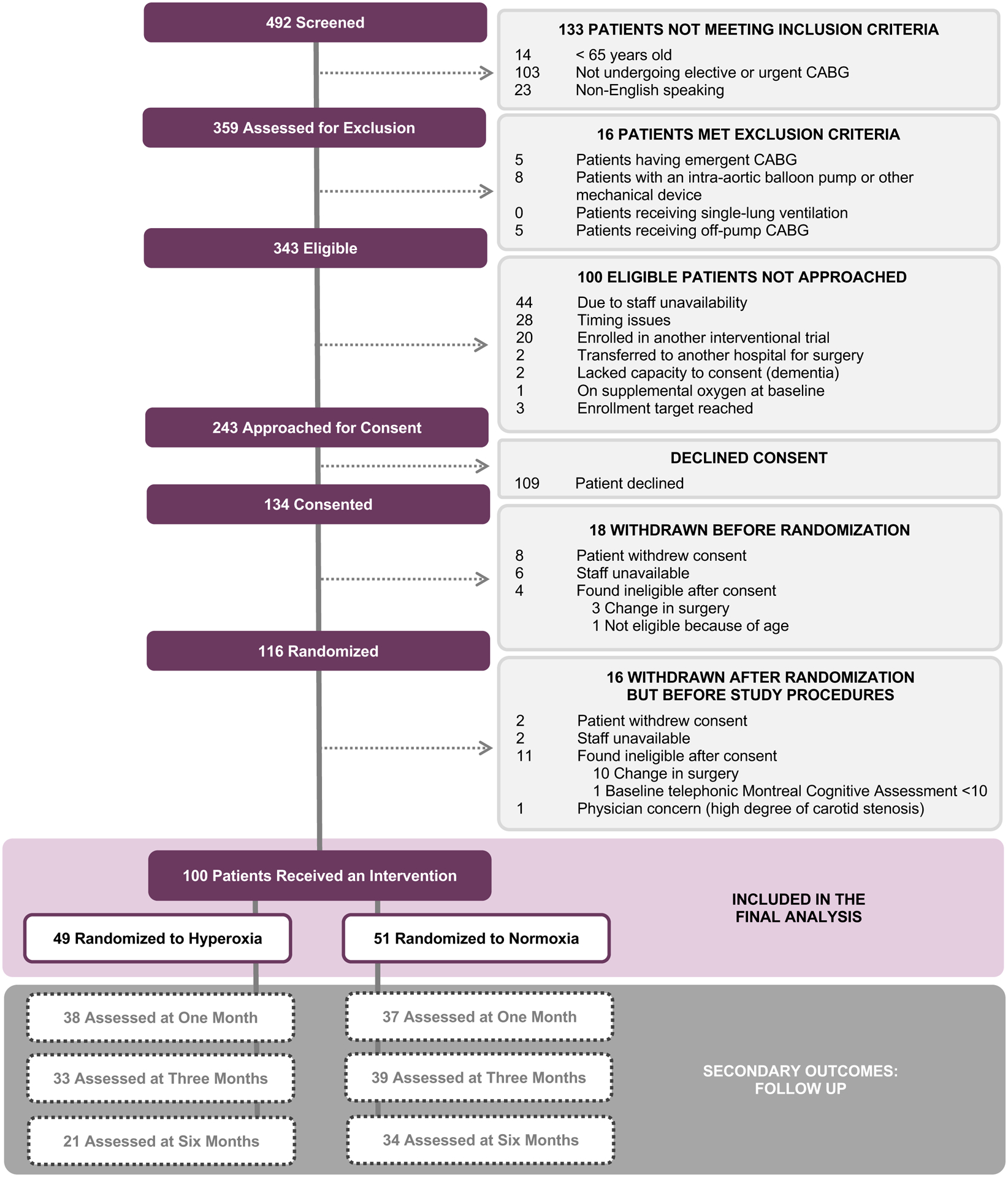
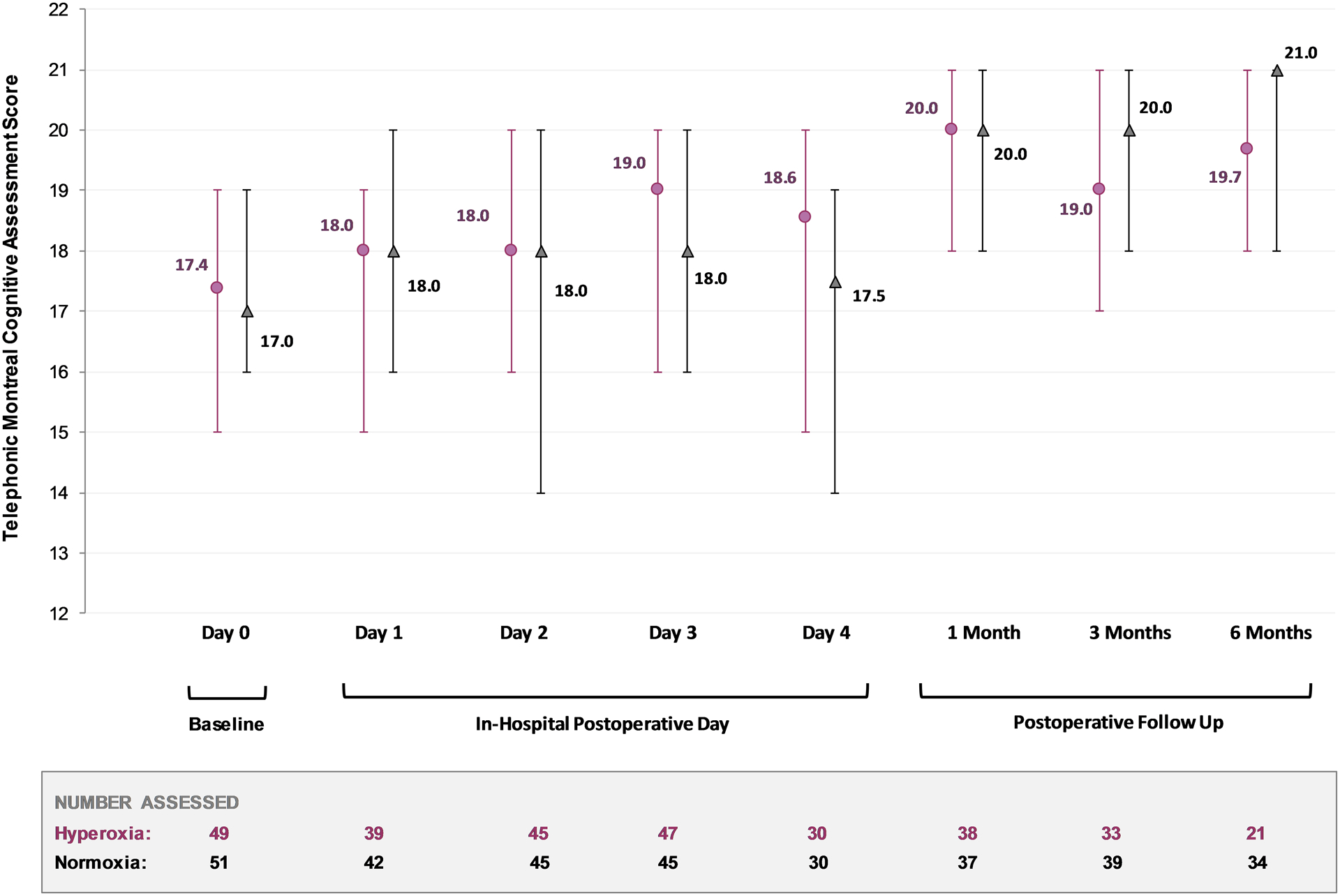
Methods: A randomized double-blind trial was conducted in patients aged 65 yr or older having coronary artery bypass graft surgery with cardiopulmonary bypass. A total of 100 patients were randomized to one of two intraoperative oxygen delivery strategies. Normoxic patients (n = 50) received a minimum fraction of inspired oxygen of 0.35 to maintain a Pao2 above 70 mmHg before and after cardiopulmonary bypass and between 100 and 150 mmHg during cardiopulmonary bypass. Hyperoxic patients (n = 50) received a fraction of inspired oxygen of 1.0 throughout surgery, irrespective of Pao2 levels. The primary outcome was neurocognitive function measured on postoperative day 2 using the Telephonic Montreal Cognitive Assessment. Secondary outcomes included neurocognitive function at 1, 3, and 6 months, as well as postoperative delirium, mortality, and durations of mechanical ventilation, intensive care unit stay, and hospital stay.
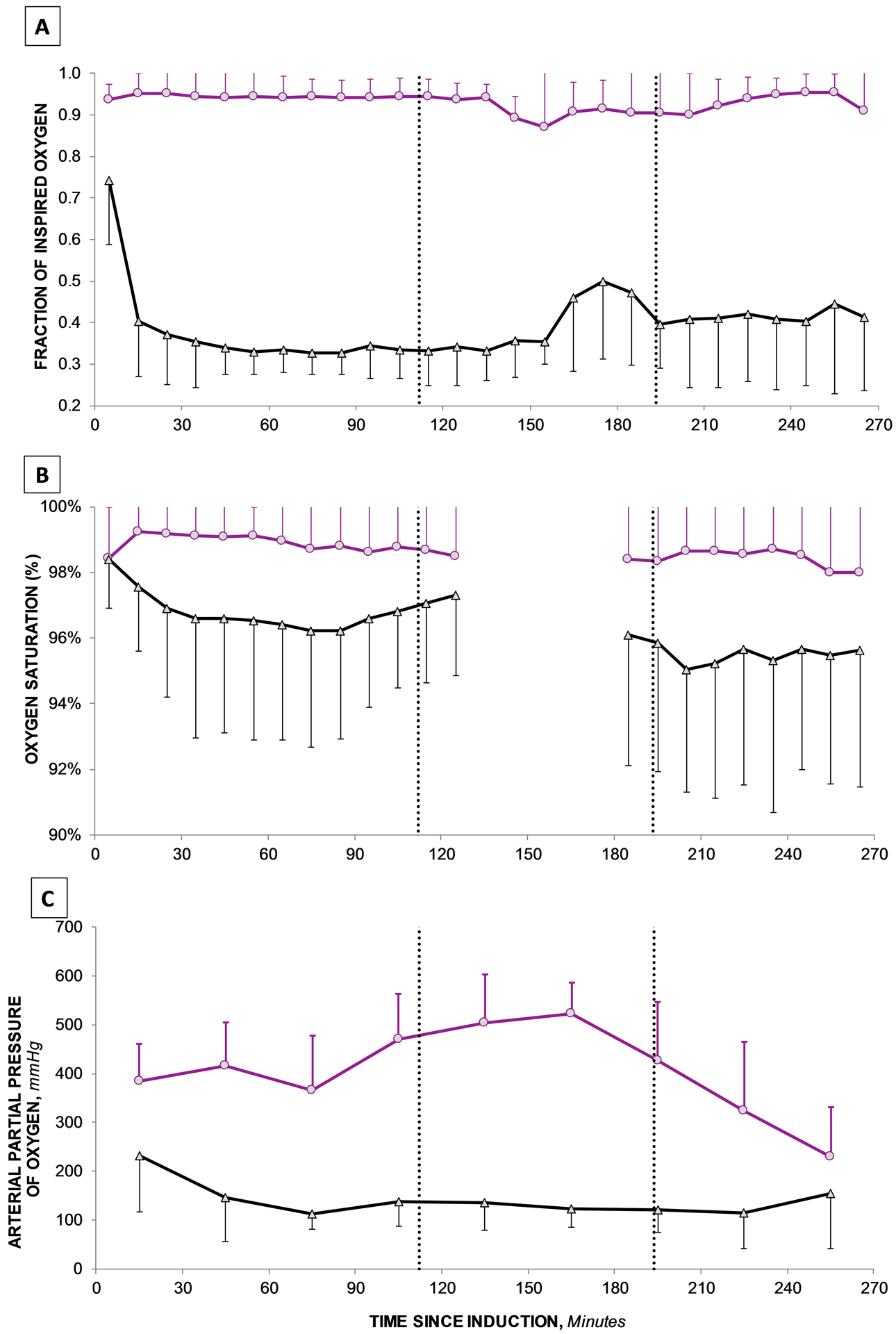
Results: The median age was 71 yr (interquartile range, 68 to 75), and the median baseline neurocognitive score was 17 (16 to 19). The median intraoperative Pao2 was 309 (285 to 352) mmHg in the hyperoxia group and 153 (133 to 168) mmHg in the normoxia group (P < 0.001). The median Telephonic Montreal Cognitive Assessment score on postoperative day 2 was 18 (16 to 20) in the hyperoxia group and 18 (14 to 20) in the normoxia group (P = 0.42). Neurocognitive function at 1, 3, and 6 months, as well as secondary outcomes, were not statistically different between groups.
Conclusions: In this randomized controlled trial, intraoperative normoxia did not reduce postoperative cognitive dysfunction when compared to intraoperative hyperoxia in older patients having cardiac surgery. Although the optimal intraoperative oxygenation strategy remains uncertain, the results indicate that intraoperative hyperoxia does not worsen postoperative cognition after cardiac surgery.
Copyright © 2020, the American Society of Anesthesiologists, Inc. All Rights Reserved.
Conflict of interest statement
Conflicts of Interest
Dr. Shaefi received speaking honorarium for University of North Carolina Visiting Professorship lecture. Ms. Mueller receives statistical consulting fees from The University of Chicago. Dr. O’ Gara receives consulting fees from Sedana Medical (Danderyd, Sweden). Dr. Bagchi receives consulting fees from Lungpacer Medical Inc (British Columbia, Canada). Ms. Banner-Goodspeed received salary support from several NIH and DoD grants, unrelated to this project. Dr. Subramaniam receives grant support from Mallinckrodt Pharmaceuticals (Staines-upon-Thames, United Kingdom) and Edward Lifesciences (Irvine CA). The other authors declare no competing interests.
Figures
References
-
- Statistics CfDCNCfH: National Hospital Discharge Survey: 2010 table, Procedures by selected patient characteristics – Number by procedure category and age, 2010
-
- Newman MF, Kirchner JL, Phillips-Bute B, Gaver V, Grocott H, Jones RH, Mark DB, Reves JG, Blumenthal JA, Neurological Outcome Research G, the Cardiothoracic Anesthesiology Research Endeavors I: Longitudinal assessment of neurocognitive function after coronary-artery bypass surgery. N Engl J Med 2001; 344: 395–402 - PubMed
-
- Phillips-Bute B, Mathew JP, Blumenthal JA, Grocott HP, Laskowitz DT, Jones RH, Mark DB, Newman MF: Association of neurocognitive function and quality of life 1 year after coronary artery bypass graft (CABG) surgery. Psychosom Med 2006; 68: 369–75 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
