

Total Body Irradiation or Chemotherapy Conditioning in Childhood ALL: A Multinational, Randomized, Noninferiority Phase III Study
- PMID: 33332189
- PMCID: PMC8078415
- DOI: 10.1200/JCO.20.02529
Total Body Irradiation or Chemotherapy Conditioning in Childhood ALL: A Multinational, Randomized, Noninferiority Phase III Study
Abstract
Purpose: Total body irradiation (TBI) before allogeneic hematopoietic stem cell transplantation (HSCT) in pediatric patients with acute lymphoblastic leukemia (ALL) is efficacious, but long-term side effects are concerning. We investigated whether preparative combination chemotherapy could replace TBI in such patients.
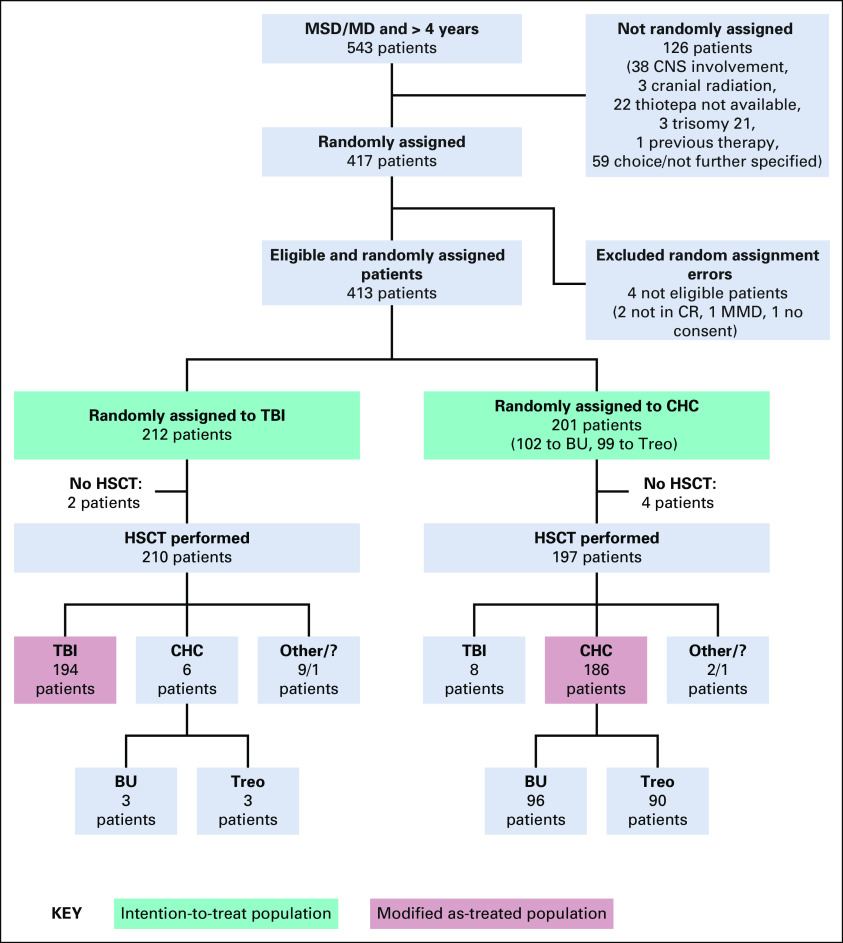
Patients and methods: FORUM is a randomized, controlled, open-label, international, multicenter, phase III, noninferiority study. Patients ≤ 18 years at diagnosis, 4-21 years at HSCT, in complete remission pre-HSCT, and with an HLA-compatible related or unrelated donor were randomly assigned to myeloablative conditioning with fractionated 12 Gy TBI and etoposide versus fludarabine, thiotepa, and either busulfan or treosulfan. The noninferiority margin was 8%. With 1,000 patients randomly assigned in 5 years, 2-year minimum follow-up, and one-sided alpha of 5%, 80% power was calculated. A futility stopping rule would halt random assignment if chemoconditioning was significantly inferior to TBI (EudraCT: 2012-003032-22; ClinicalTrials.gov: NCT01949129).
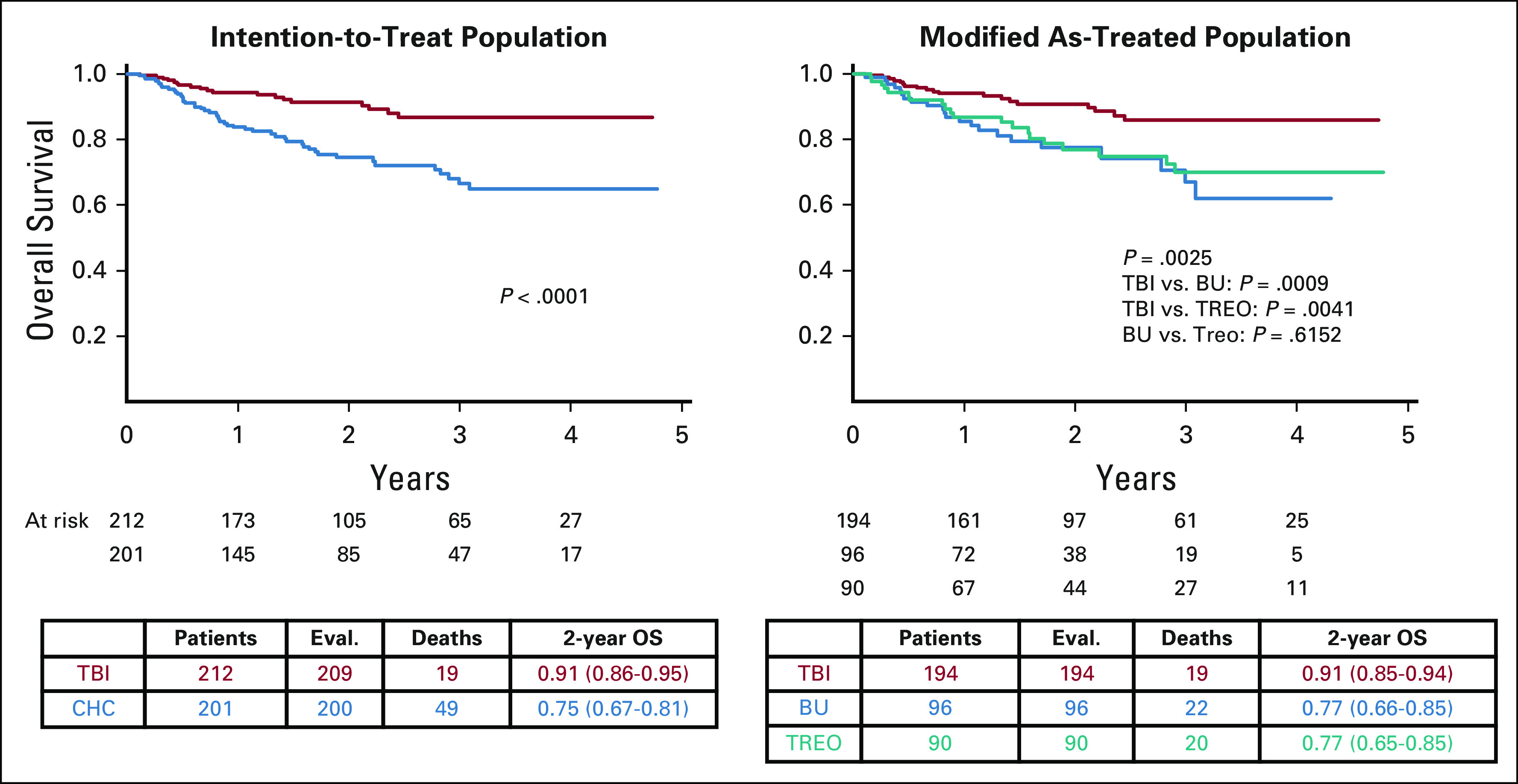
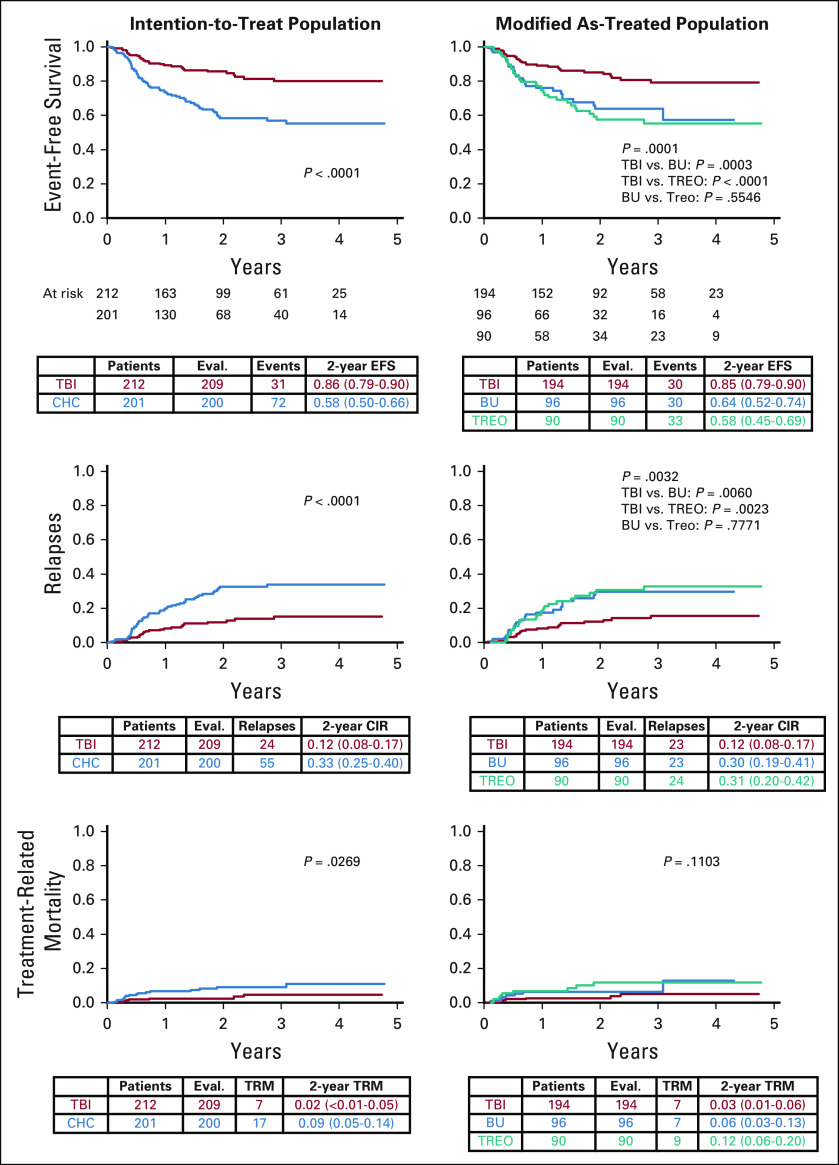
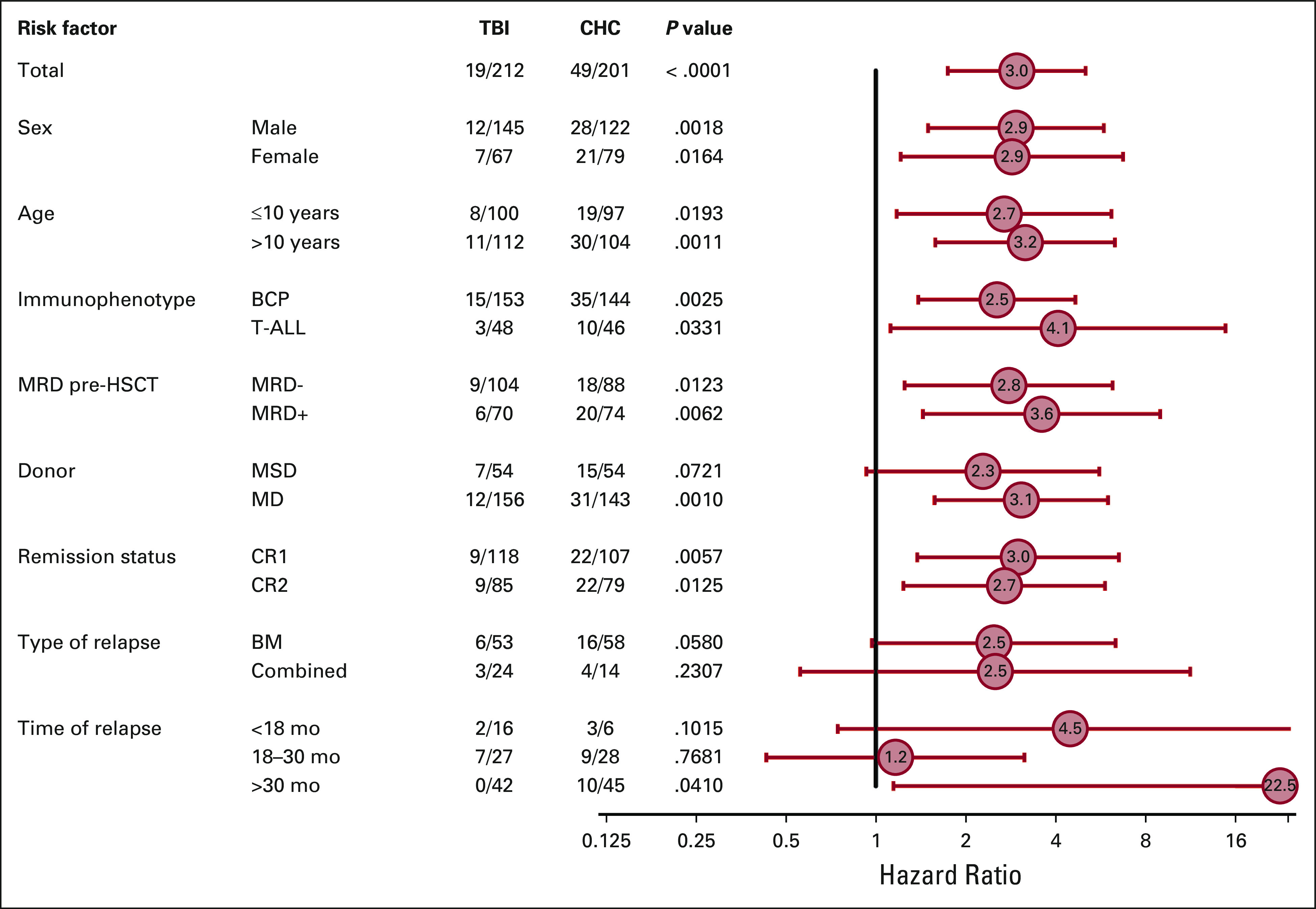
Results: Between April 2013 and December 2018, 543 patients were screened, 417 were randomly assigned, 212 received TBI, and 201 received chemoconditioning. The stopping rule was applied on March 31, 2019. The median follow-up was 2.1 years. In the intention-to-treat population, 2-year overall survival (OS) was significantly higher following TBI (0.91; 95% CI, 0.86 to 0.95; P < .0001) versus chemoconditioning (0.75; 95% CI, 0.67 to 0.81). Two-year cumulative incidence of relapse and treatment-related mortality were 0.12 (95% CI, 0.08 to 0.17; P < .0001) and 0.02 (95% CI, < 0.01 to 0.05; P = .0269) following TBI and 0.33 (95% CI, 0.25 to 0.40) and 0.09 (95% CI, 0.05 to 0.14) following chemoconditioning, respectively.
Conclusion: Improved OS and lower relapse risk were observed following TBI plus etoposide compared with chemoconditioning. We therefore recommend TBI plus etoposide for patients > 4 years old with high-risk ALL undergoing allogeneic HSCT.
Figures
Comment in
-
Continued Role for Radiation in the Conditioning Regimen for Children With ALL.J Clin Oncol. 2021 Feb 1;39(4):262-264. doi: 10.1200/JCO.20.03261. Epub 2020 Dec 17. J Clin Oncol. 2021. PMID: 33332188 No abstract available.
-
[Total body irradiation or chemotherapy conditioning in childhood ALL : A multinational, randomized, noninferiority phase III study].Strahlenther Onkol. 2021 Sep;197(9):857-858. doi: 10.1007/s00066-021-01805-1. Epub 2021 Jul 2. Strahlenther Onkol. 2021. PMID: 34213570 Free PMC article. German. No abstract available.
References
-
- Friend BD Bailey-Olson M Melton A, et al. : The impact of total body irradiation-based regimens on outcomes in children and young adults with acute lymphoblastic leukemia undergoing allogeneic hematopoietic stem cell transplantation. Pediatr Blood Cancer 67:e28079, 2020 - PubMed
-
- Hill-Kayser CE Plastaras JP Tochner Z, et al. : TBI during BM and SCT: Review of the past, discussion of the present and consideration of future directions. Bone Marrow Transplant 46:475-484, 2011 - PubMed
-
- Balduzzi A Dalle JH Wachowiak J, et al. : Transplantation in children and adolescents with acute lymphoblastic leukemia from a matched donor versus an HLA-identical sibling: Is the outcome comparable? Results from the International BFM ALL SCT 2007 Study. Biol Blood Marrow Transplant 25:2197-2210, 2019 - PubMed
-
- Dopfer R Henze G Bender-Gotze C, et al. : Allogeneic bone marrow transplantation for childhood acute lymphoblastic leukemia in second remission after intensive primary and relapse therapy according to the BFM- and CoALL-protocols: Results of the German Cooperative Study. Blood 78:2780-2784, 1991 - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
