

Radical Cystectomy Against Intravesical BCG for High-Risk High-Grade Nonmuscle Invasive Bladder Cancer: Results From the Randomized Controlled BRAVO-Feasibility Study
- PMID: 33332191
- PMCID: PMC8078404
- DOI: 10.1200/JCO.20.01665
Radical Cystectomy Against Intravesical BCG for High-Risk High-Grade Nonmuscle Invasive Bladder Cancer: Results From the Randomized Controlled BRAVO-Feasibility Study
Abstract
Purpose: High-grade nonmuscle invasive bladder cancer (HRNMIBC) is a heterogeneous disease. Treatments include intravesical maintenance Bacillus Calmette-Guerin (mBCG) and radical cystectomy (RC). We wanted to understand whether a randomized trial comparing these options was possible.
Materials and methods: We conducted a two-arm, prospective multicenter randomized study to determine the feasibility in Bacillus Calmette-Guerin-naive patients. Participants had new high-risk HRNMIBC suitable for both treatments. Random assignment was stratified by age, sex, center, stage, presence of carcinoma in situ, and prior low-risk bladder cancer. Qualitative work investigated how to maintain equipoise. The primary outcome was the number of patients screened, eligible, recruited, and randomly assigned.
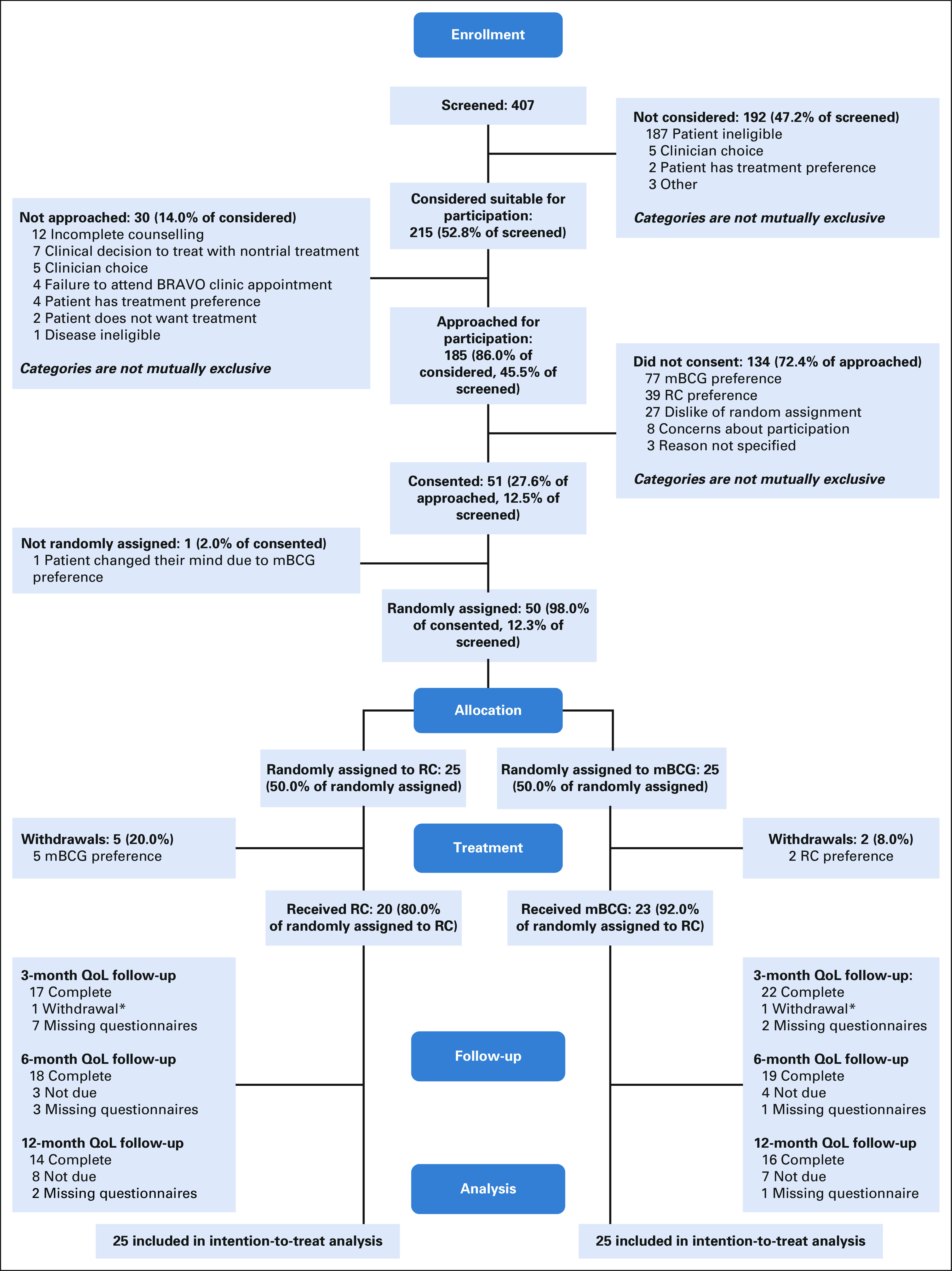
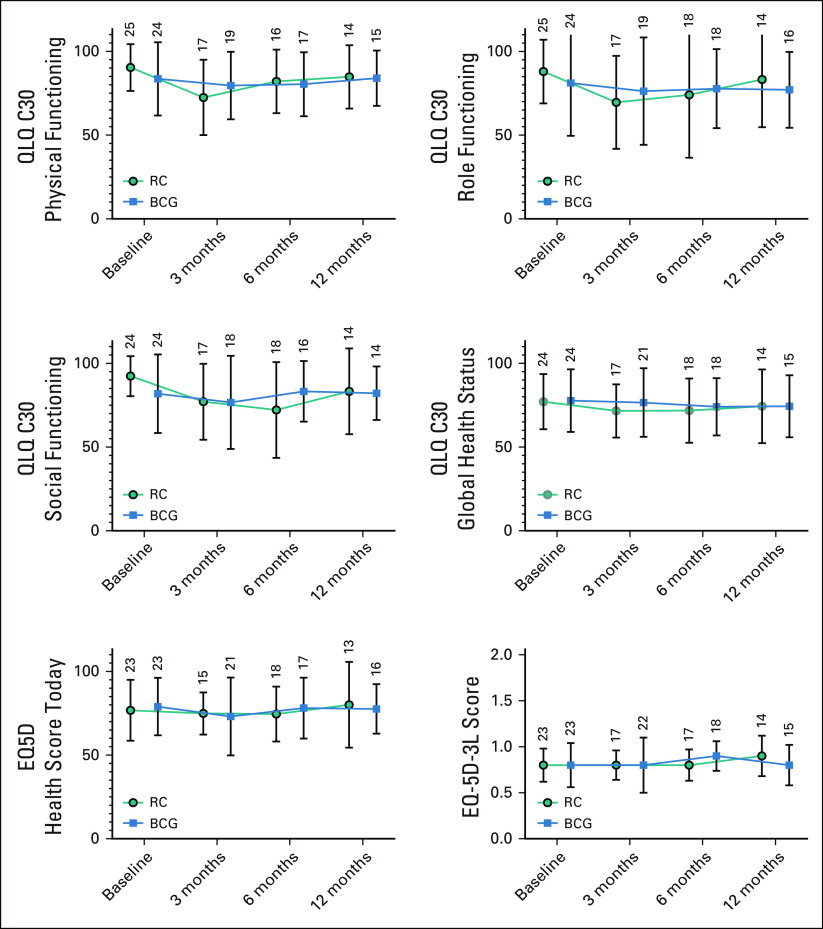
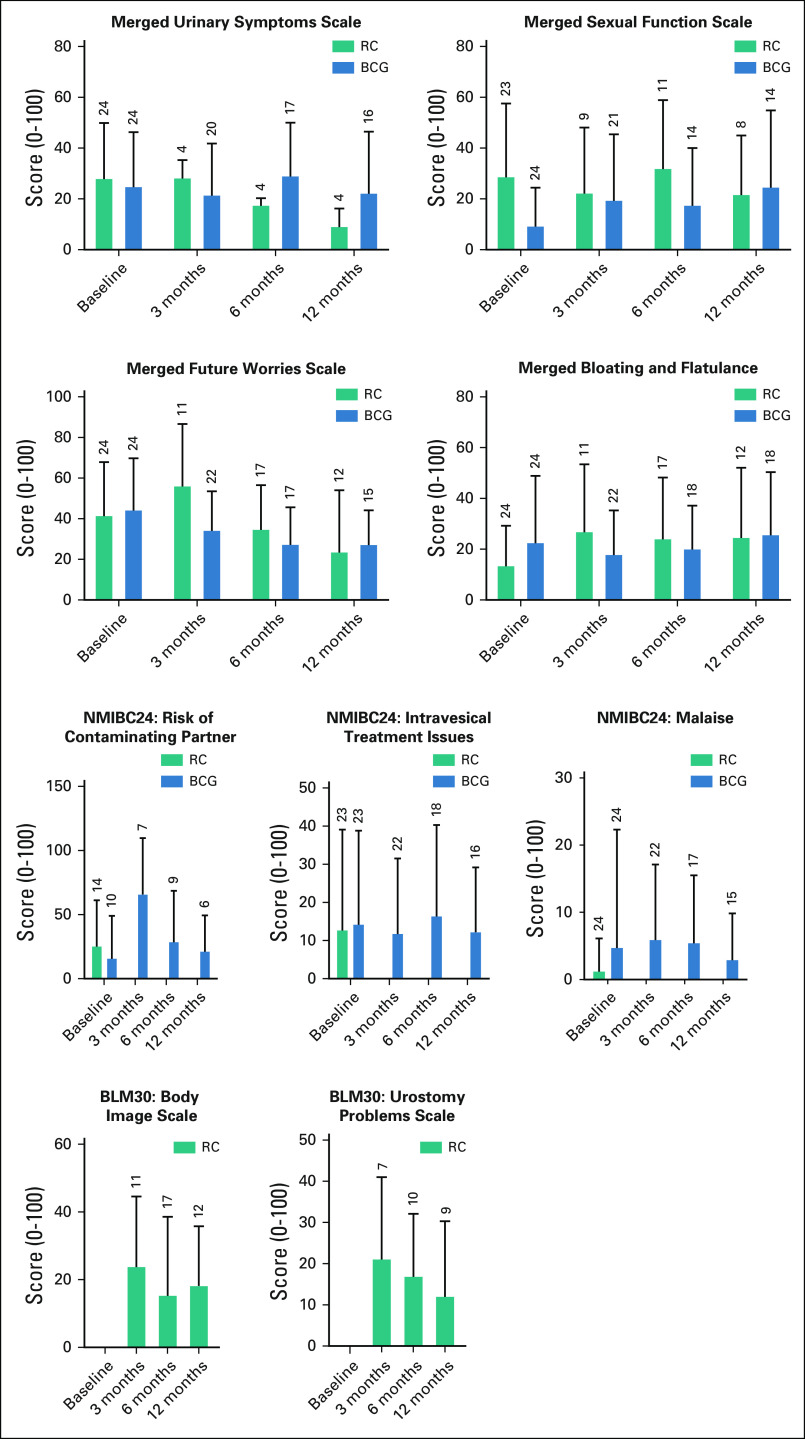
Results: We screened 407 patients, approached 185, and obtained consent from 51 (27.6%) patients. Of these, one did not proceed and therefore 50 were randomly assigned (1:1). In the mBCG arm, 23/25 (92.0%) patients received mBCG, four had nonmuscle invasive bladder cancer (NMIBC) after induction, three had NMIBC at 4 months, and four received RC. At closure, two patients had metastatic BC. In the RC arm, 20 (80.0%) participants received cystectomy, including five (25.0%) with no tumor, 13 (65.0%) with HRNMIBC, and two (10.0%) with muscle invasion in their specimen. At follow-up, all patients in the RC arm were free of disease. Adverse events were mostly mild and equally distributed (15/23 [65.2%] patients with mBCG and 13/20 [65.0%] patients with RC). The quality of life (QOL) of both arms was broadly similar at 12 months.
Conclusion: A randomized controlled trial comparing mBCG and RC will be challenging to recruit into. Around 10% of patients with high-risk HRNMIBC have a lethal disease and may be better treated by primary radical treatment. Conversely, many are suitable for bladder preservation and may maintain their prediagnosis QOL.
Figures
Comment in
-
Re: Radical Cystectomy Against Intravesical BCG for High-risk High-grade Nonmuscle Invasive Bladder Cancer: Results from the Randomized Controlled BRAVO-feasibility Study.Eur Urol. 2021 Sep;80(3):386-387. doi: 10.1016/j.eururo.2021.05.034. Epub 2021 Jun 24. Eur Urol. 2021. PMID: 34175150 No abstract available.
-
Re: Radical Cystectomy Against Intravesical BCG for High-Risk High-Grade Nonmuscle Invasive Bladder Cancer: Results From the Randomized Controlled BRAVO-Feasibility Study.Eur Urol. 2022 Apr;81(4):430. doi: 10.1016/j.eururo.2022.01.011. Epub 2022 Jan 31. Eur Urol. 2022. PMID: 35094897 No abstract available.
-
Urological Oncology: Bladder, Penis and Urethral Cancer, and Basic Principles of Oncology.J Urol. 2022 Jun;207(6):1346-1348. doi: 10.1097/JU.0000000000002650. Epub 2022 Mar 23. J Urol. 2022. PMID: 35319252 No abstract available.
References
-
- Cumberbatch MGK Jubber I Black PC, et al. : Epidemiology of bladder cancer: A systematic review and contemporary update of risk factors in 2018. Eur Urol 74:784-795, 2018 - PubMed
-
- Leal J Luengo-Fernandez R Sullivan R, et al. : Economic burden of bladder cancer across the European Union. Eur Urol 69:438-447, 2016 - PubMed
-
- Sylvester RJ van der Meijden AP Oosterlinck W, et al. : Predicting recurrence and progression in individual patients with stage Ta T1 bladder cancer using EORTC risk tables: a combined analysis of 2596 patients from seven EORTC trials. Eur Urol 49:466-475, 2006; discussion 475-477 - PubMed
-
- Thomas F Noon AP Rubin N, et al. : Comparative outcomes of primary, recurrent, and progressive high-risk non-muscle-invasive bladder cancer. Eur Urol 63:145-154, 2013 - PubMed
-
- Babjuk M Burger M Comperat EM, et al. : European association of urology guidelines on non-muscle-invasive bladder cancer (TaT1 and carcinoma in Situ)—2019 update. Eur Urol 76:639-657, 2019 - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
