

Comparison of Protective Effects of Recombinant Antithrombin Gamma and Plasma-Derived Antithrombin on Sepsis-Induced Disseminated Intravascular Coagulation and Multiple Organ Failure
- PMID: 33332196
- PMCID: PMC7750769
- DOI: 10.1177/1076029620981630
Comparison of Protective Effects of Recombinant Antithrombin Gamma and Plasma-Derived Antithrombin on Sepsis-Induced Disseminated Intravascular Coagulation and Multiple Organ Failure
Abstract
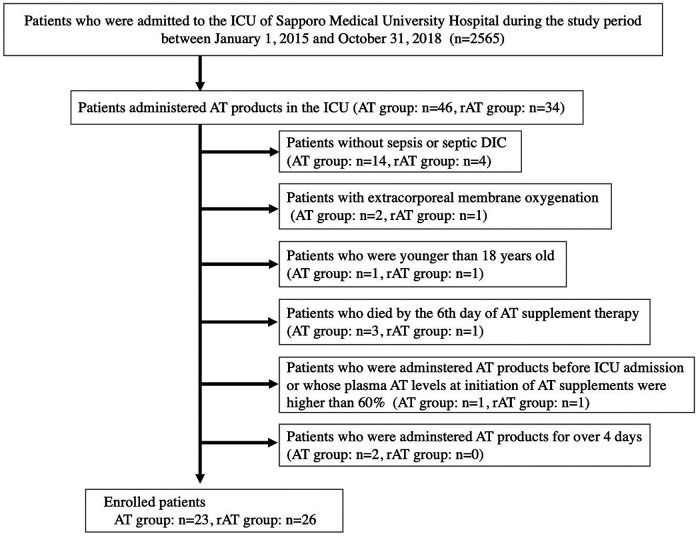
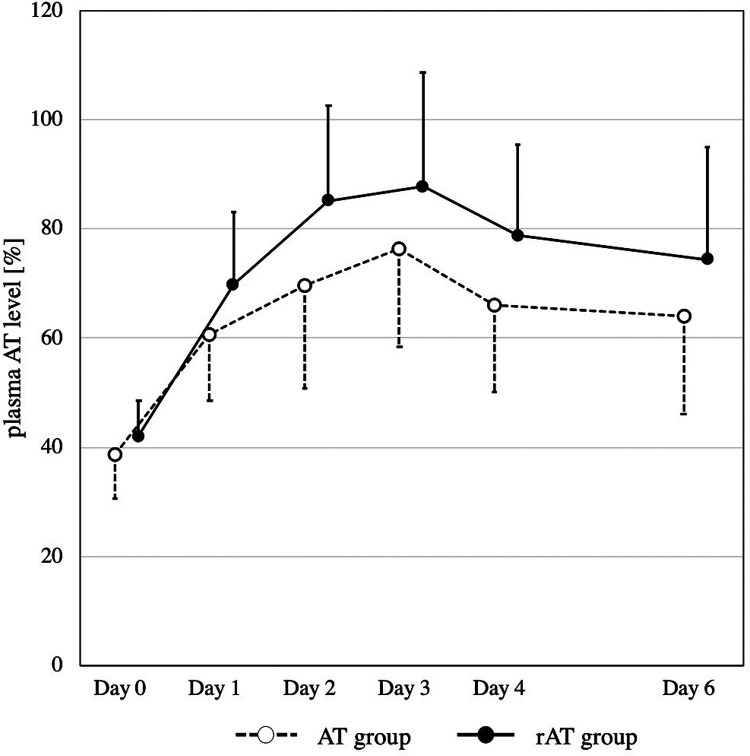
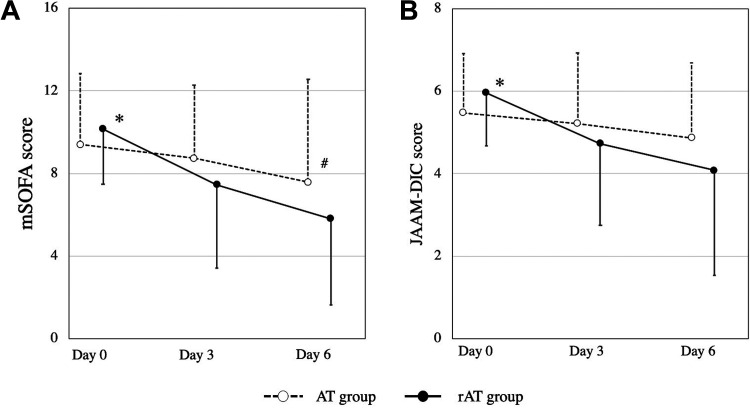
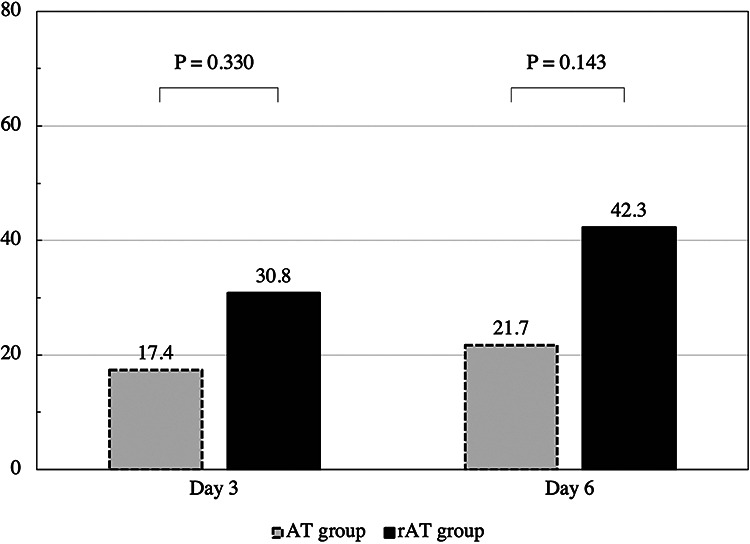
In Japan, the dose of the new recombinant antithrombin III concentrate (rAT-gamma) is titrated according to patient body weight (BW), while conventional plasma-derived antithrombin concentrates (AT) are administered as a fixed dose. Therefore, it is anticipated that rAT-gamma could produce better treatment effects than AT. The aim of this study was to compare the organ protective effects of doses of rAT-gamma and AT administered in clinical practice for septic disseminated intravascular coagulation (DIC) and multiple organ failure. This study was performed at a single university hospital in Japan. A total of 49 patients with antithrombin deficiency secondary to septic DIC who were administered either rAT-gamma (n = 26) or AT (n = 23) were retrospectively analyzed to assess the dose of supplemental antithrombin concentrates, plasma antithrombin activity, Japanese Association for Acute Medicine (JAAM)-DIC score, and modified Sequential Organ Failure Assessment (SOFA) score on days 0, 3 and 6. The AT-equivalent dose per kg BW of rAT-gamma (equal to the initial rAT-gamma dose per kg BW divided by 1.2) was significantly higher than the dose per kg BW of AT (AT 23.4 ± 5.1 vs. rAT 28.9 ± 3.9 IU/kg/day; P < 0.001). Consequently, serial increases in plasma antithrombin levels occurred more rapidly in the rAT-gamma group (P = 0.036). JAAM DIC and modified SOFA scores revealed significantly greater improvement in the rAT versus the AT group (JAAM DIC score: P = 0.042, mSOFA score: P = 0.005). The results of this study suggest that AT supplementation adjusted for patient BW might further improve septic DIC and multiple organ failure.
Keywords: antithrombin III; disseminated intravascular coagulation; recombinant antithrombin gamma; sepsis; sequential organ failure assessment score.
Conflict of interest statement
Figures
References
-
- Semeraro N, Ammollo CT, Semeraro F, Colucci M. Sepsis, thrombosis and organ dysfunction. Thromb Res. 2012;129(3):290–295. - PubMed
-
- Levi M, Ten Cate H. Disseminated intravascular coagulation. N Engl J Med. 1999;341:586–592. - PubMed
-
- Opal SM. Interactions between coagulation and inflammation. Scand J Infect Dis. 2003;35(9):545–554. - PubMed
-
- Levi M, Poll TV. Coagulation in patients with severe sepsis. Semin Thromb Hemost. 2015;41(1):9–15. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
