

Transcriptomic and proteomic intra-tumor heterogeneity of colorectal cancer varies depending on tumor location within the colorectum
- PMID: 33332369
- PMCID: PMC7746197
- DOI: 10.1371/journal.pone.0241148
Transcriptomic and proteomic intra-tumor heterogeneity of colorectal cancer varies depending on tumor location within the colorectum
Abstract
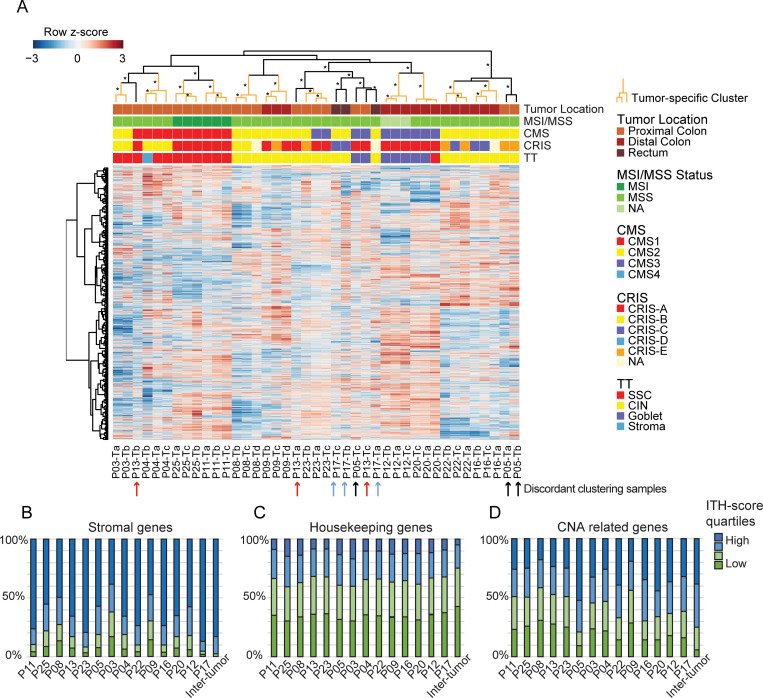
Background: Intra-tumor heterogeneity (ITH) of colorectal cancer (CRC) complicates molecular tumor classification, such as transcriptional subtyping. Differences in cellular states, biopsy cell composition, and tumor microenvironment may all lead to ITH. Here we analyze ITH at the transcriptomic and proteomic levels to ascertain whether subtype discordance between multiregional biopsies reflects relevant biological ITH or lack of classifier robustness. Further, we study the impact of tumor location on ITH.
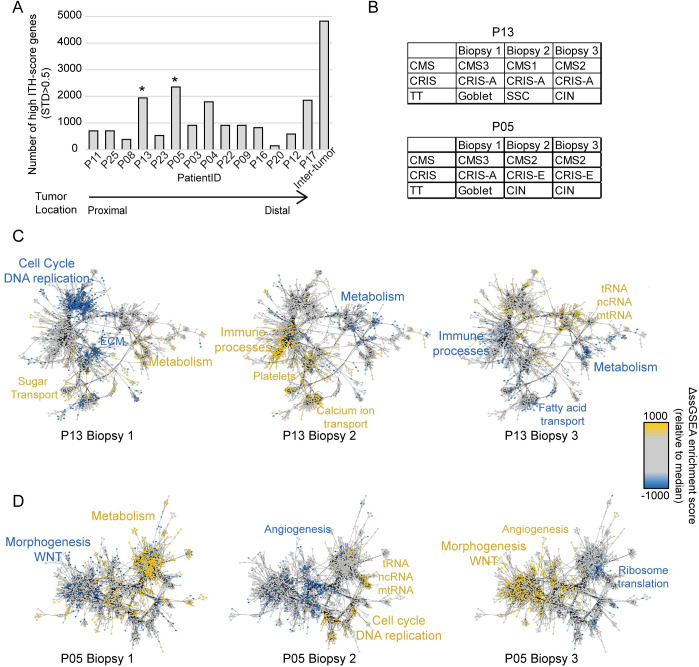
Methods: Multiregional biopsies from stage II and III CRC tumors were analyzed by RNA sequencing (41 biopsies, 14 tumors) and multiplex immune protein analysis (89 biopsies, 29 tumors). CRC subtyping was performed using consensus molecular subtypes (CMS), CRC intrinsic subtypes (CRIS), and TUMOR types. ITH-scores and network maps were defined to determine the origin of heterogeneity. A validation cohort was used with one biopsy per tumor (162 tumors).
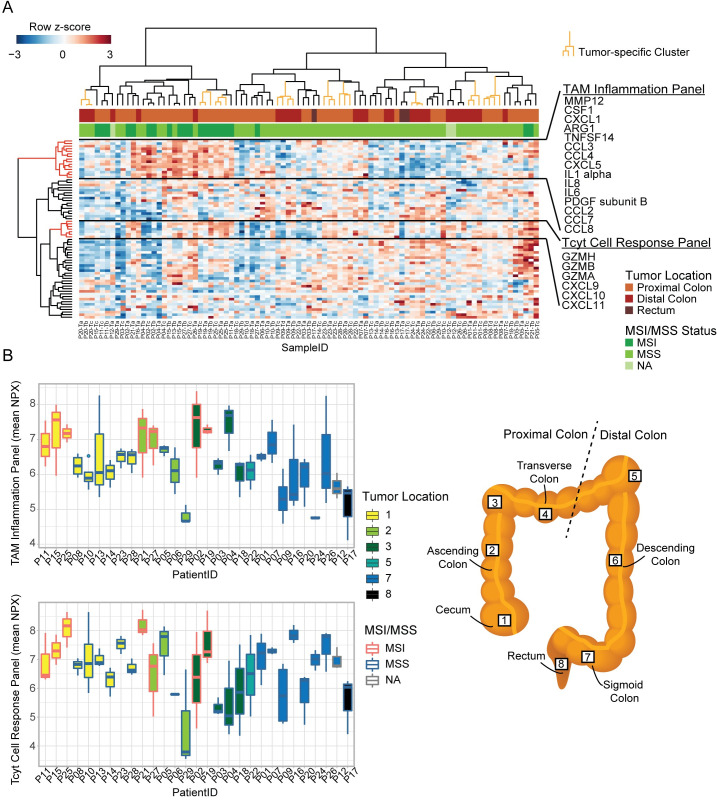
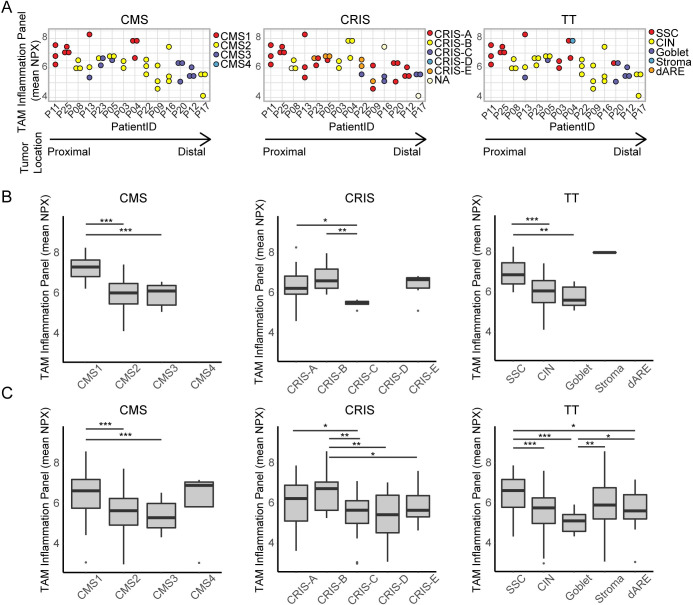
Results: Overall, inter-tumor transcriptional variation exceeded ITH, and subtyping calls were frequently concordant between multiregional biopsies. Still, some tumors had high transcriptional ITH and were classified discordantly. Subtyping of proximal MSS tumors were discordant for 50% of the tumors, this ITH was related to differences in the microenvironment. Subtyping of distal MSS tumors were less discordant, here the ITH was more cancer-cell related. The subtype discordancy reflected actual molecular ITH within the tumors. The relevance of the subtypes was reflected at protein level where several inflammation markers were significantly increased in immune related transcriptional subtypes, which was verified in an independent cohort (Wilcoxon rank sum test; p<0.05). Unsupervised hierarchical clustering of the protein data identified large ITH at protein level; as the multiregional biopsies clustered together for only 9 out of 29 tumors.
Conclusion: Our transcriptomic and proteomic analyses show that the tumor location along the colorectum influence the ITH of CRC, which again influence the concordance of subtyping.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures

References
-
- Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA: a cancer journal for clinicians. 2018;68(6):394–424. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
