

Inflammation initiates a vicious cycle between obesity and nonalcoholic fatty liver disease
- PMID: 33332766
- PMCID: PMC7860600
- DOI: 10.1002/iid3.391
Inflammation initiates a vicious cycle between obesity and nonalcoholic fatty liver disease
Abstract
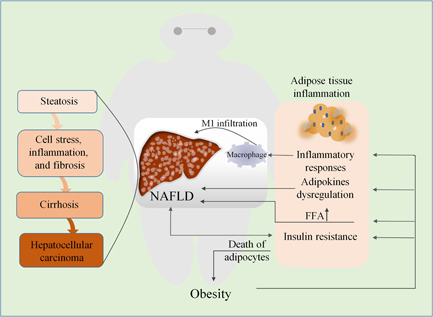
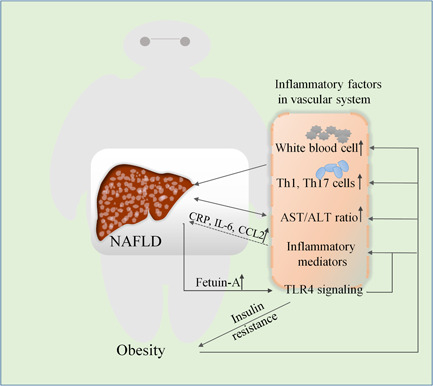
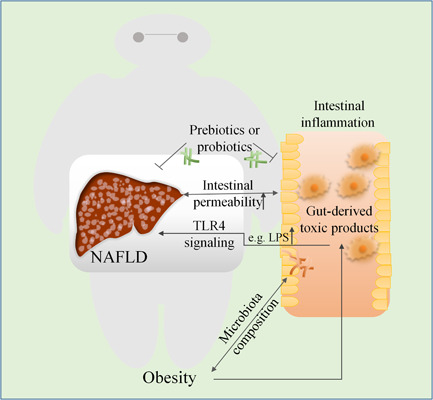
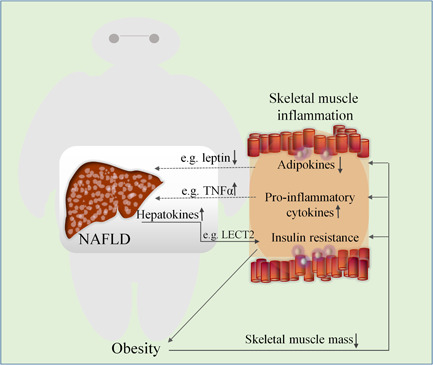
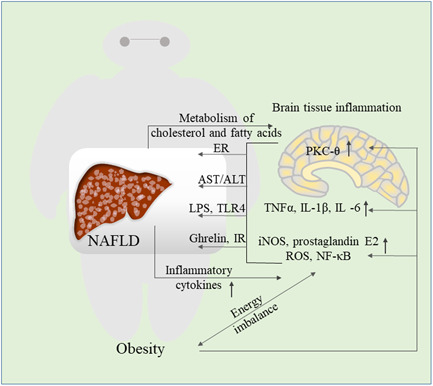
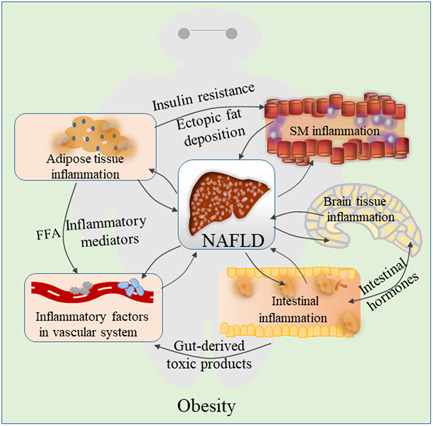
Low-level of chronic inflammation activation is characteristic of obesity. Nonalcoholic fatty liver disease (NAFLD) is closely linked to obesity and is an emerging health problem, it originates from abnormal accumulation of triglycerides in the liver, and sometimes causes inflammatory reactions that could contribute to cirrhosis and liver cancer, thus its pathogenesis needs to be clarified for more treatment options. Once NAFLD is established, it contributes to systemic inflammation, the low-grade inflammation is continuously maintained during NAFLD causing impaired resolution of inflammation in obesity, which subsequently exacerbates its severity. This study focuses on the effects of obesity-induced inflammations, which are the underlying causes of the disease progression and development of more severe inflammatory and fibrotic stages. Understanding the relationship between obesity and NAFLD could help in establishing attractive therapeutic targets or diagnostic markers in obesity-induced inflammation response and provides new approaches for the prevention and treatment of NAFLD in obesity.
Keywords: NAFLD; adipose tissue inflammation; obesity; obesity-induced inflammation.
© 2020 The Authors. Immunity, Inflammation and Disease published by John Wiley & Sons Ltd.
Conflict of interest statement
The authors declare that there are no conflict of interests.
Figures
References
-
- Hill JJ. Obesity: an emerging threat. J Natl Black Nurses Assoc. 2018;29:36‐39. - PubMed
-
- Lukaszewski MA, Eberle D, Vieau D, Breton C. Nutritional manipulations in the perinatal period program adipose tissue in offspring. Am J Physiol Endocrinol Metab. 2013;305:E1195‐E1207. - PubMed
-
- Polyzos SA, Kountouras J, Mantzoros CS. Obesity and nonalcoholic fatty liver disease: from pathophysiology to therapeutics. Metabolism. 2019;92:82‐97. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
