Real-Time Light-Guided Vocal Fold Injection: An In Vivo Feasibility Study in a Canine Model
- PMID: 33332956
- PMCID: PMC8373830
- DOI: 10.21053/ceo.2020.02180
Real-Time Light-Guided Vocal Fold Injection: An In Vivo Feasibility Study in a Canine Model
Abstract
Objectives: The transcutaneous approach is a good option for office-based vocal fold injection (VFI). However, precise localization requires extensive experience because the needle tip is invisible in small and complex laryngeal spaces. Recently, real-time light-guided VFI (RL-VFI) was proposed as a new technique that allows simultaneous injection under precise needle localization by light guidance. Herein, we aimed to verify the feasibility of RL-VFI in an in vivo canine model and explored its clinical usefulness.
Methods: The device for RL-VFI comprised a light source (light-emitting diode modules [10 W] of red color [650 nm]) and injectors (1.5 inches, 23 gauge). An adult male beagle was used for the experiment. After tracheostomy, a rigid laryngoscope was inserted and suspended to expose the larynx. A flexible naso-laryngoscopy system was used to visualize the vocal folds.
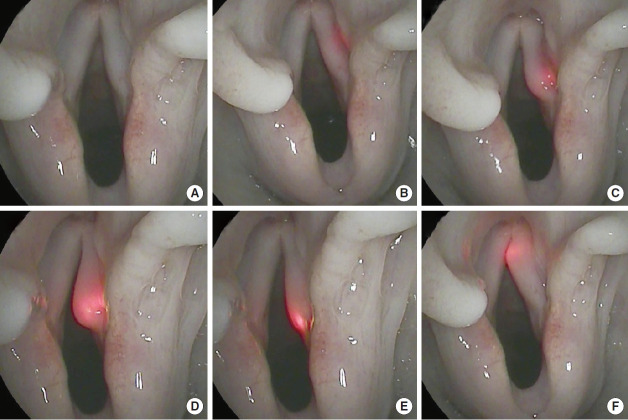
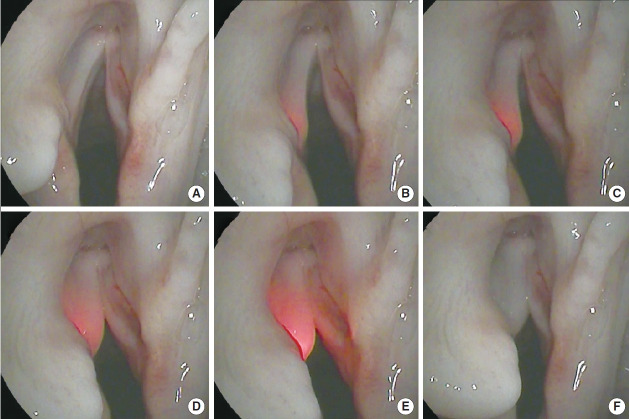
Results: RL-VFI was performed using various transcutaneous approaches, including the cricothyroid, transthyroid, and transhyoid approaches. Light guidance helped identify the path of the needle and prevent inadvertent penetration. The location of the needle tip was accurately indicated by the light. The illuminated needle could be easily placed at the intended points in the vocal fold with real-time visual-motor feedback. Hyaluronic acid could be simultaneously injected lateral to the vocal process under light guidance without manipulation of the device.
Conclusion: RL-VFI was found to be safe and feasible in an in vivo canine model, providing precise localization and visualmotor feedback. The clinical application of RL-VFI is expected to improve the safety and precision of VFI.
Keywords: In Vivo Animal Study; Real-Time Light-Guided Vocal Fold Injection; Transcutaneous Approach; Vocal Fold Injection; Vocal Fold Palsy.
Conflict of interest statement
The corresponding author (WC) is the inventor of the device. Pusan National University and Pusan National University Hospital hold the patents related to the device, granted by the Korean Intellectual Property Office (KR101699229B1), the Patent Cooperation Treaty (WO2017039193A1), and United States Patent and Trademark Office (US15/536,419). The authors have no other funding or financial relationship to disclose.
Figures





References
-
- Rosen CA, Amin MR, Sulica L, Simpson CB, Merati AL, Courey MS, et al. Advances in office-based diagnosis and treatment in laryngology. Laryngoscope. 2009 Nov;119 Suppl 2:S185–212. - PubMed
-
- Kwon TK, Buckmire R. Injection laryngoplasty for management of unilateral vocal fold paralysis. Curr Opin Otolaryngol Head Neck Surg. 2004 Dec;12(6):538–42. - PubMed
-
- Cha W, Ro JH, Wang SG, Jang JY, Cho JK, Kim GH, et al. Development of a device for real-time light-guided vocal fold injection: a preliminary report. Laryngoscope. 2016 Apr;126(4):936–40. - PubMed
-
- Cha W, Ro JH, Yang SC, Choi CJ, Yang I, Kang H, et al. Real-time light-guided vocal fold injection: ex vivo feasibility study in a canine model. Laryngoscope. 2019 Apr;129(4):935–42. - PubMed