

Inflammatory Endotype-associated Airway Microbiome in Chronic Obstructive Pulmonary Disease Clinical Stability and Exacerbations: A Multicohort Longitudinal Analysis
- PMID: 33332995
- PMCID: PMC8483235
- DOI: 10.1164/rccm.202009-3448OC
Inflammatory Endotype-associated Airway Microbiome in Chronic Obstructive Pulmonary Disease Clinical Stability and Exacerbations: A Multicohort Longitudinal Analysis
Abstract
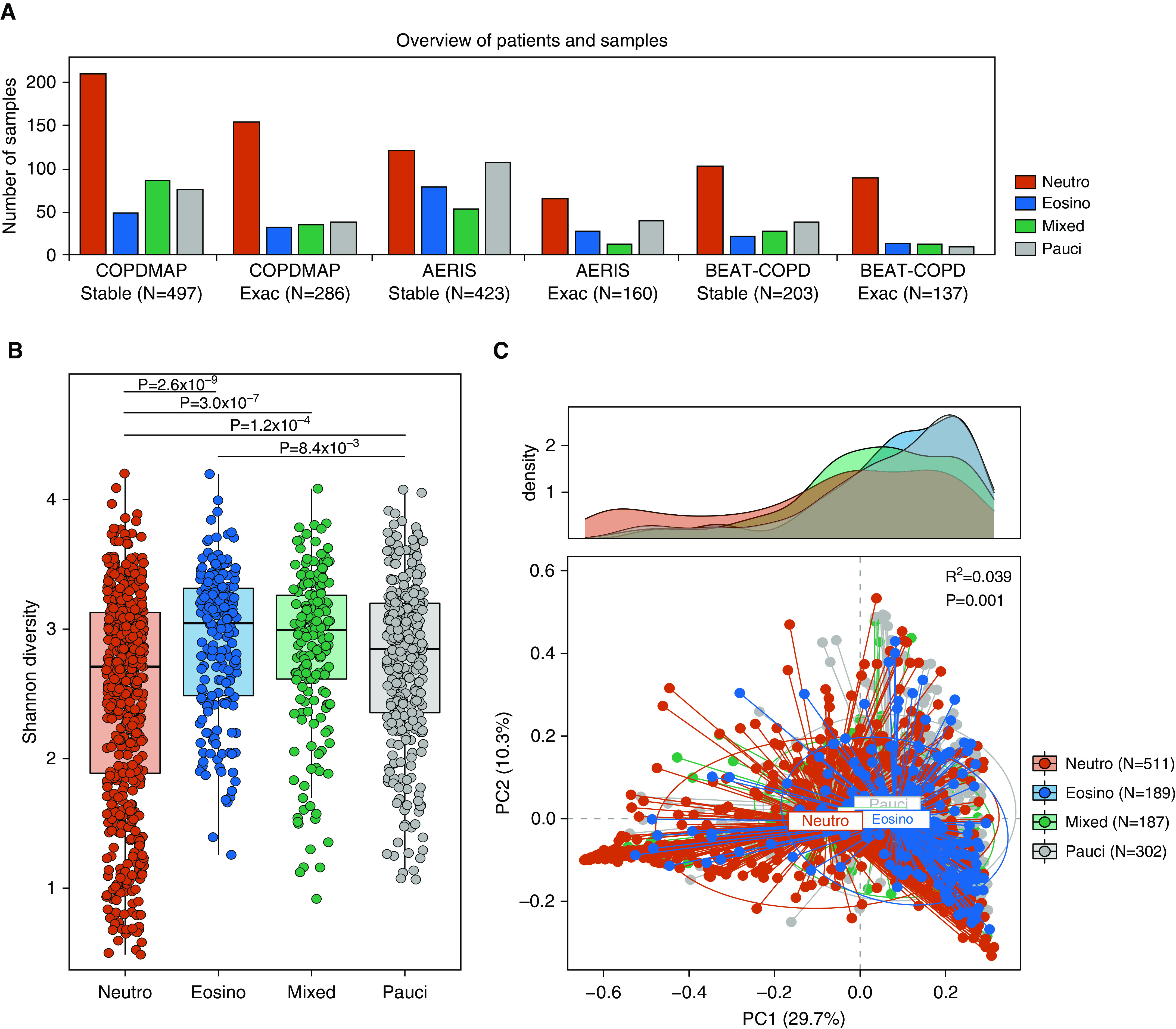
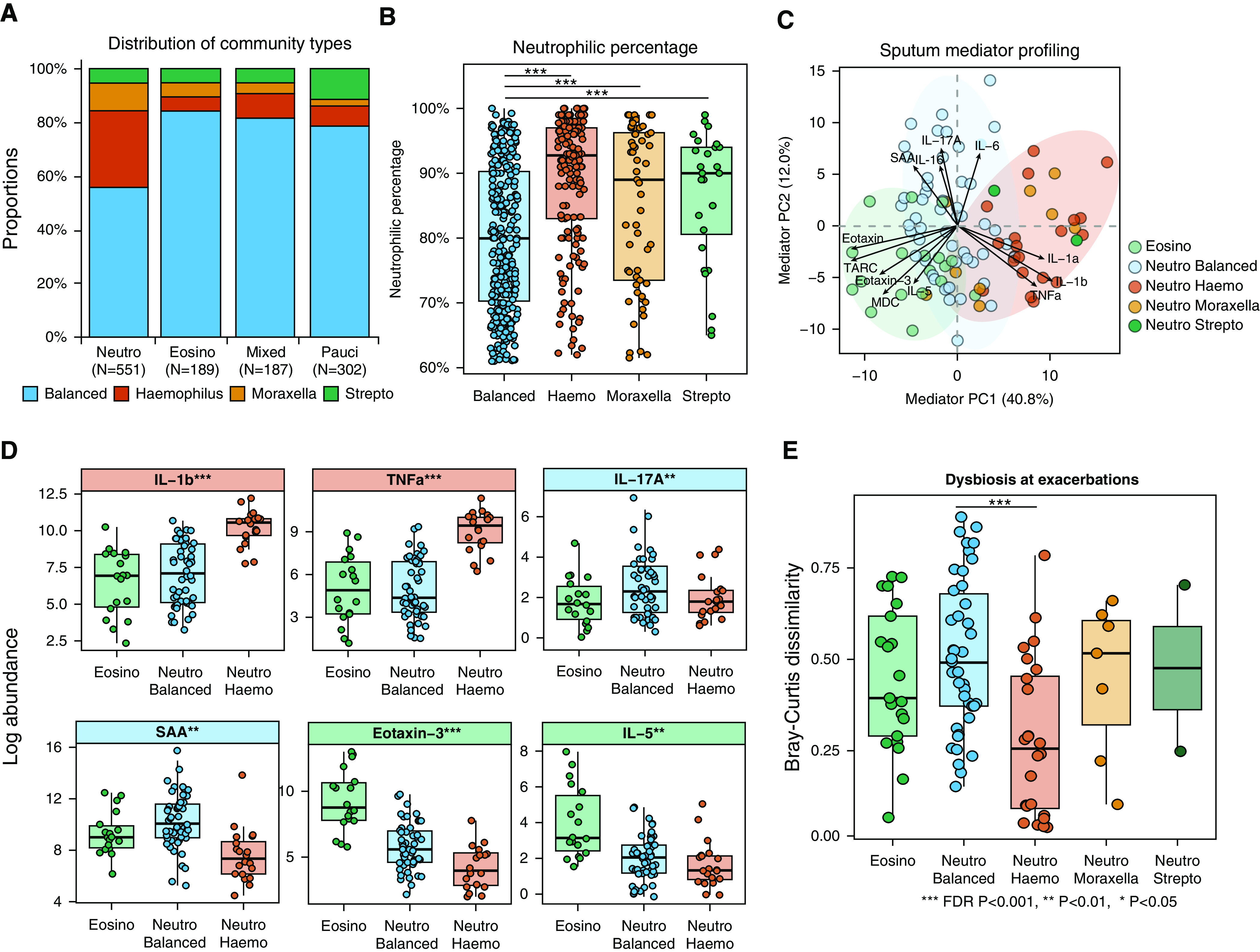
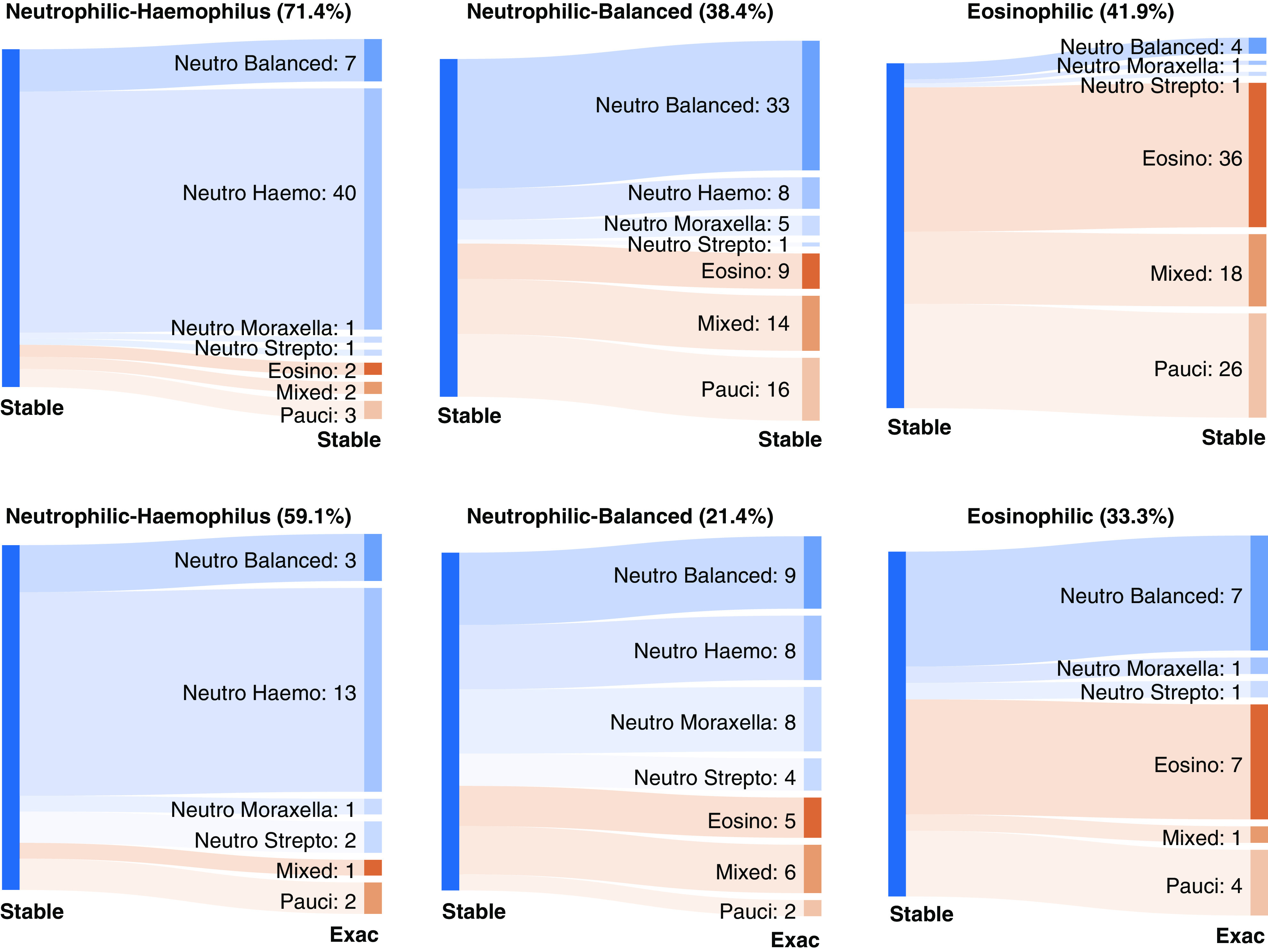
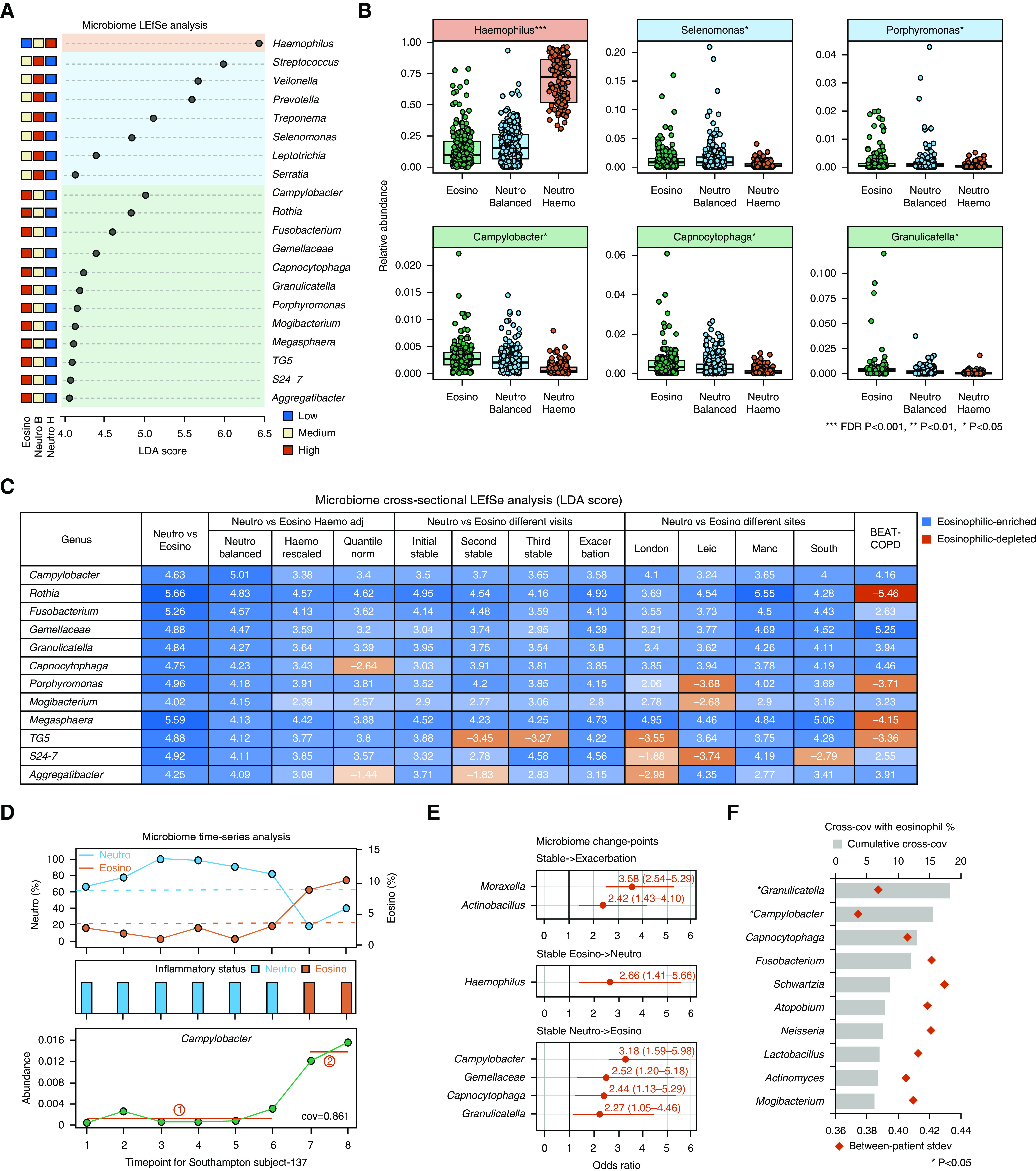
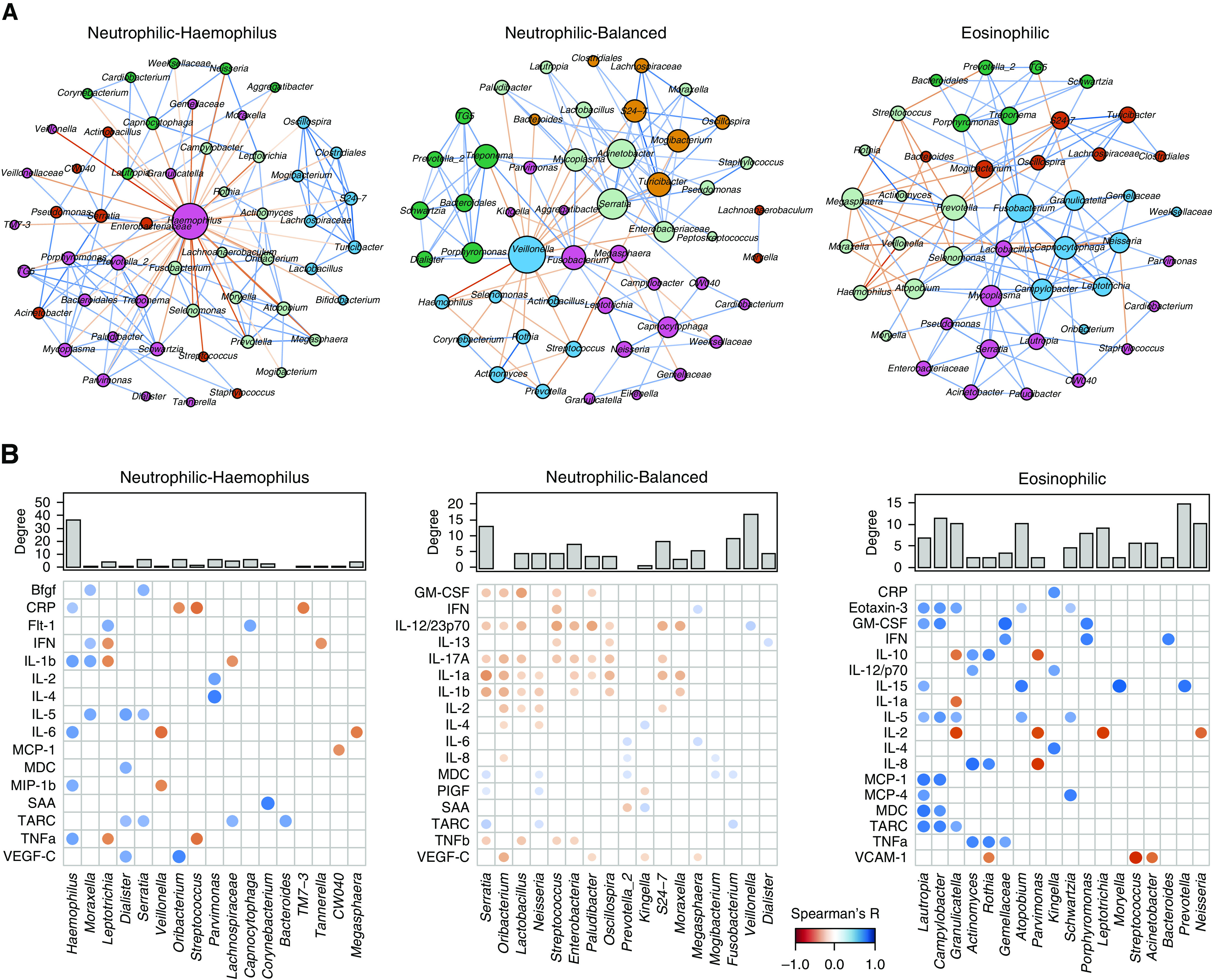
Rationale: Understanding the role of the airway microbiome in chronic obstructive pulmonary disease (COPD) inflammatory endotypes may help to develop microbiome-based diagnostic and therapeutic approaches. Objectives: To understand the association of the airway microbiome with neutrophilic and eosinophilic COPD at stability and during exacerbations. Methods: An integrative analysis was performed on 1,706 sputum samples collected longitudinally from 510 patients with COPD recruited at four UK sites of the BEAT-COPD (Biomarkers to Target Antibiotic and Systemic COPD), COPDMAP (Chronic Obstructive Pulmonary Disease Medical Research Council/Association of the British Pharmaceutical Industry), and AERIS (Acute Exacerbation and Respiratory Infections in COPD) cohorts. The microbiome was analyzed using COPDMAP and AERIS as a discovery data set and BEAT-COPD as a validation data set. Measurements and Main Results: The airway microbiome in neutrophilic COPD was heterogeneous, with two primary community types differentiated by the predominance of Haemophilus. The Haemophilus-predominant subgroup had elevated sputum IL-1β and TNFα (tumor necrosis factor α) and was relatively stable over time. The other neutrophilic subgroup with a balanced microbiome profile had elevated sputum and serum IL-17A and was temporally dynamic. Patients in this state at stability were susceptible to the greatest microbiome shifts during exacerbations. This subgroup can temporally switch to both neutrophilic Haemophilus-predominant and eosinophilic states that were otherwise mutually exclusive. Time-series analysis on the microbiome showed that the temporal trajectories of Campylobacter and Granulicatella were indicative of intrapatient switches from neutrophilic to eosinophilic inflammation, in track with patient sputum eosinophilia over time. Network analysis revealed distinct host-microbiome interaction patterns among neutrophilic Haemophilus-predominant, neutrophilic balanced microbiome, and eosinophilic subgroups. Conclusions: The airway microbiome can stratify neutrophilic COPD into subgroups that justify different therapies. Neutrophilic and eosinophilic COPD are interchangeable in some patients. Monitoring temporal variability of the airway microbiome may track patient inflammatory status over time.
Keywords: airway microbiome; chronic obstructive pulmonary disease; cytokines; inflammatory endotypes; unbiased clusters.
Figures
Comment in
-
Crossing Kingdoms: Host-Microbial Endotyping and the Quest to Understand Treatable Traits in Chronic Obstructive Pulmonary Disease.Am J Respir Crit Care Med. 2021 Jun 15;203(12):1447-1448. doi: 10.1164/rccm.202101-0169ED. Am J Respir Crit Care Med. 2021. PMID: 33651664 Free PMC article. No abstract available.
References
-
- Bach PB, Brown C, Gelfand SE, McCrory DC. American College of Physicians–American Society of Internal Medicine; American College of Chest Physicians. Management of acute exacerbations of chronic obstructive pulmonary disease: a summary and appraisal of published evidence. Ann Intern Med. 2001;134:600–620. PubMed - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
