

Lead-Time Trajectory of CA19-9 as an Anchor Marker for Pancreatic Cancer Early Detection
- PMID: 33333055
- PMCID: PMC8783758
- DOI: 10.1053/j.gastro.2020.11.052
Lead-Time Trajectory of CA19-9 as an Anchor Marker for Pancreatic Cancer Early Detection
Abstract
Background & aims: There is substantial interest in liquid biopsy approaches for cancer early detection among subjects at risk, using multi-marker panels. CA19-9 is an established circulating biomarker for pancreatic cancer; however, its relevance for pancreatic cancer early detection or for monitoring subjects at risk has not been established.
Methods: CA19-9 levels were assessed in blinded sera from 175 subjects collected up to 5 years before diagnosis of pancreatic cancer and from 875 matched controls from the Prostate, Lung, Colorectal and Ovarian (PLCO) Cancer Screening Trial. For comparison of performance, CA19-9 was assayed in blinded independent sets of samples collected at diagnosis from 129 subjects with resectable pancreatic cancer and 275 controls (100 healthy subjects; 50 with chronic pancreatitis; and 125 with noncancerous pancreatic cysts). The complementary value of 2 additional protein markers, TIMP1 and LRG1, was determined.
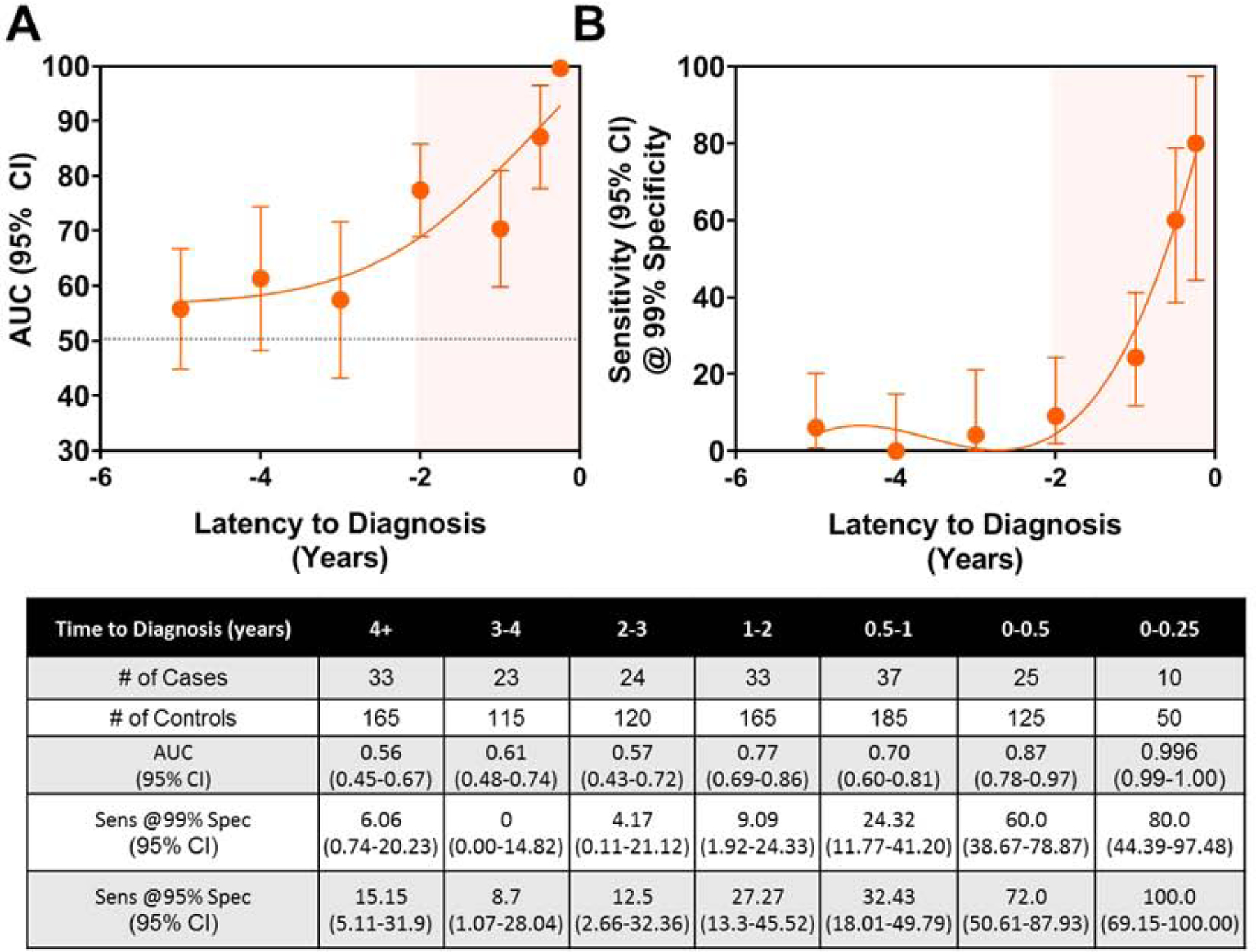
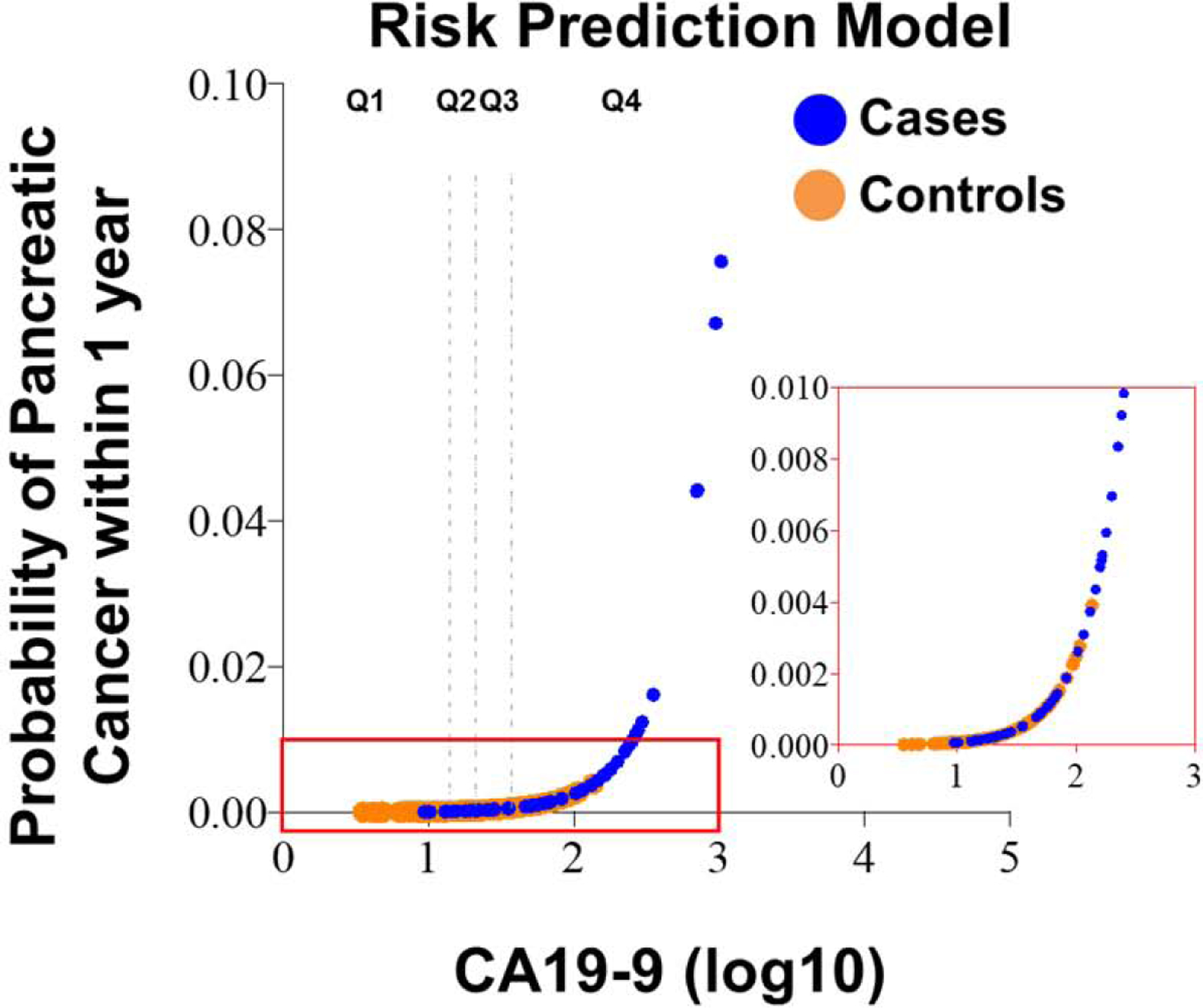
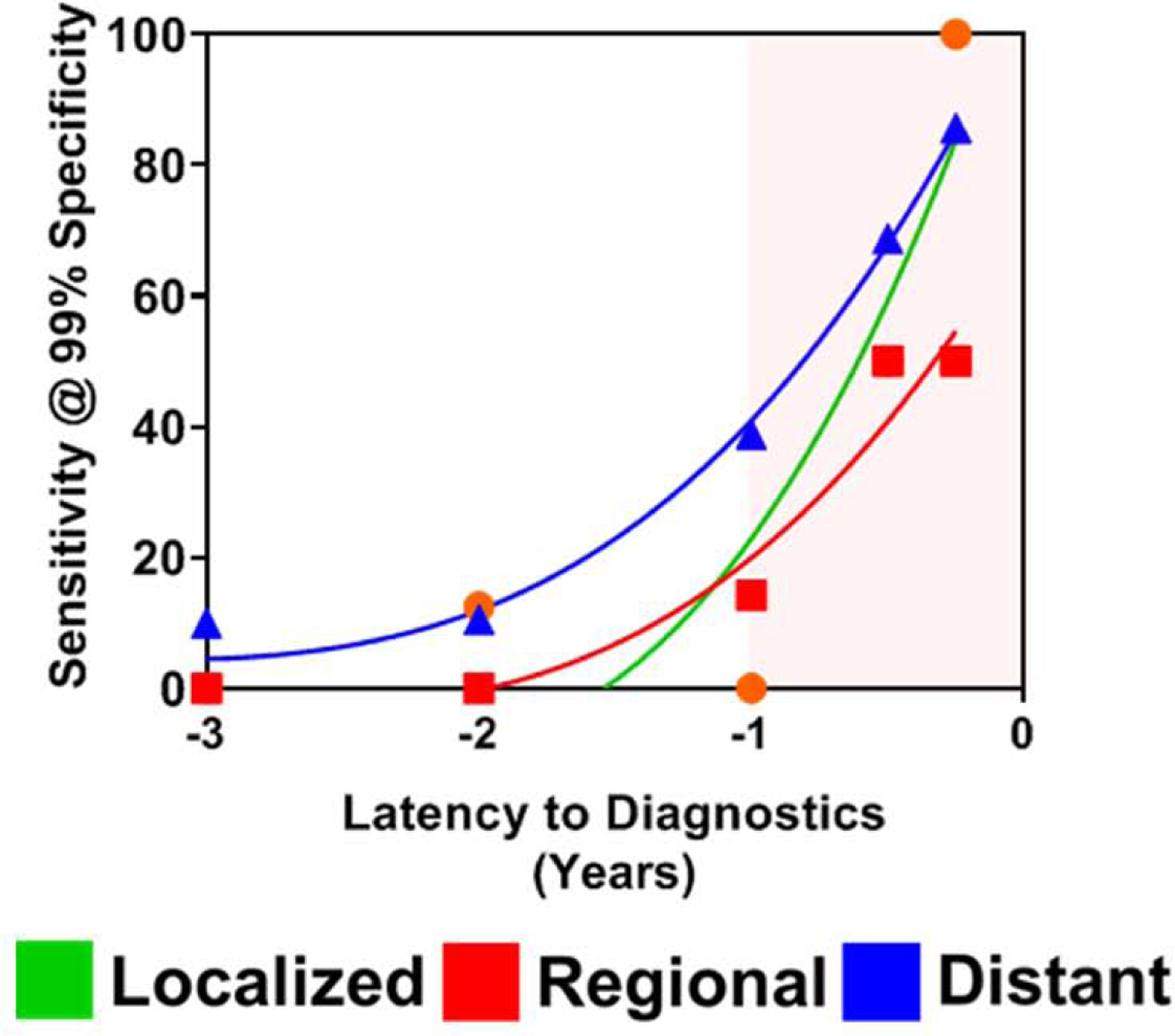
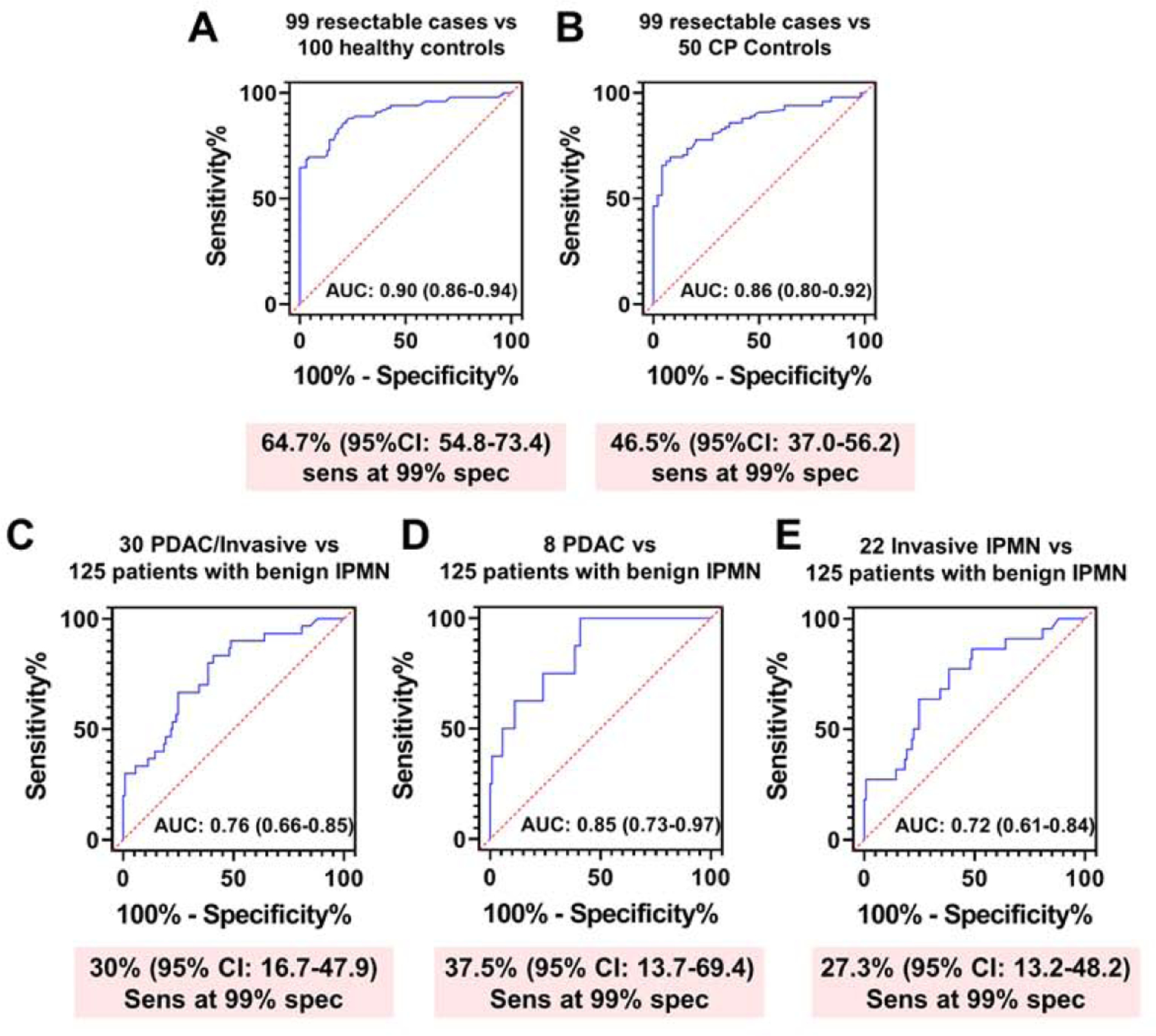
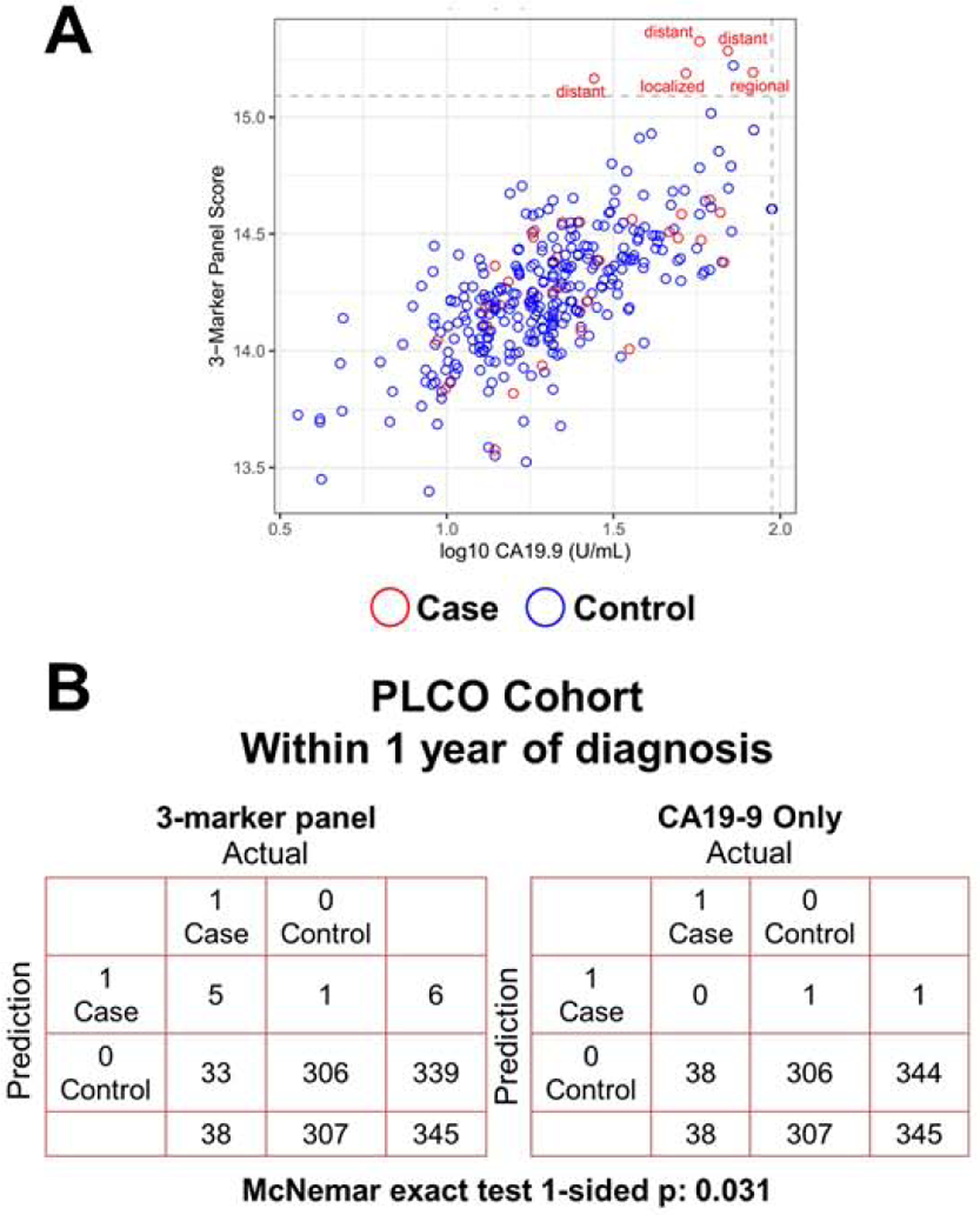
Results: In the PLCO cohort, levels of CA19-9 increased exponentially starting at 2 years before diagnosis with sensitivities reaching 60% at 99% specificity within 0 to 6 months before diagnosis for all cases and 50% at 99% specificity for cases diagnosed with early-stage disease. Performance was comparable for distinguishing newly diagnosed cases with resectable pancreatic cancer from healthy controls (64% sensitivity at 99% specificity). Comparison of resectable pancreatic cancer cases to subjects with chronic pancreatitis yielded 46% sensitivity at 99% specificity and for subjects with noncancerous cysts, 30% sensitivity at 99% specificity. For prediagnostic cases below cutoff value for CA19-9, the combination with LRG1 and TIMP1 yielded an increment of 13.2% in sensitivity at 99% specificity (P = .031) in identifying cases diagnosed within 1 year of blood collection.
Conclusion: CA19-9 can serve as an anchor marker for pancreatic cancer early detection applications.
Keywords: Biomarker; Detection; Pancreatic Cancer.
Copyright © 2021 AGA Institute. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Old Dog, New Tricks: Use of CA 19-9 for Early Diagnosis of Pancreatic Cancer.Gastroenterology. 2021 Mar;160(4):1019-1021. doi: 10.1053/j.gastro.2021.01.001. Epub 2021 Jan 5. Gastroenterology. 2021. PMID: 33417931 No abstract available.
References
-
- Ryan DP, Hong TS, Bardeesy N. Pancreatic adenocarcinoma. N Engl J Med 2014;371:1039–49. - PubMed
-
- Kleeff J, Korc M, Apte M, et al. Pancreatic cancer. Nat Rev Dis Primers 2016;2:16022. - PubMed
-
- Neoptolemos JP, Kleeff J, Michl P, et al. Therapeutic developments in pancreatic cancer: current and future perspectives. Nat Rev Gastroenterol Hepatol 2018;15:333–348. - PubMed
-
- Cloyd JM, Katz MH, Prakash L, et al. Preoperative Therapy and Pancreatoduodenectomy for Pancreatic Ductal Adenocarcinoma: a 25-Year Single-Institution Experience. J Gastrointest Surg 2017;21:164–174. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
