

Data quality of the routine health management information system at the primary healthcare facility and district levels in Tanzania
- PMID: 33334323
- PMCID: PMC7745510
- DOI: 10.1186/s12911-020-01366-w
Data quality of the routine health management information system at the primary healthcare facility and district levels in Tanzania
Abstract
Background: Effective planning for disease prevention and control requires accurate, adequately-analysed, interpreted and communicated data. In recent years, efforts have been put in strengthening health management information systems (HMIS) in Sub-Saharan Africa to improve data accessibility to decision-makers. This study assessed the quality of routine HMIS data at primary healthcare facility (HF) and district levels in Tanzania.
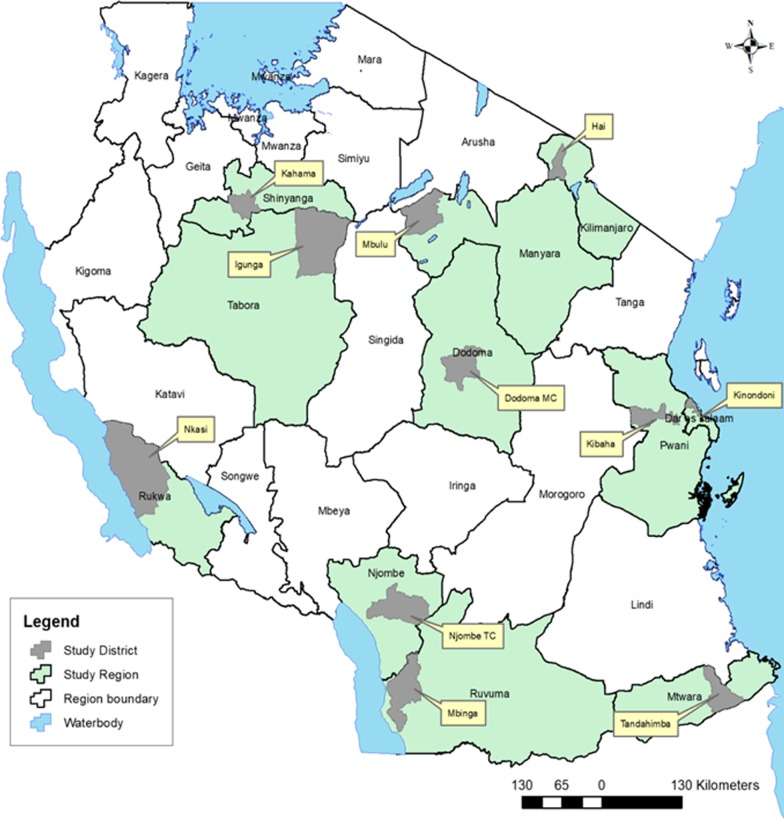
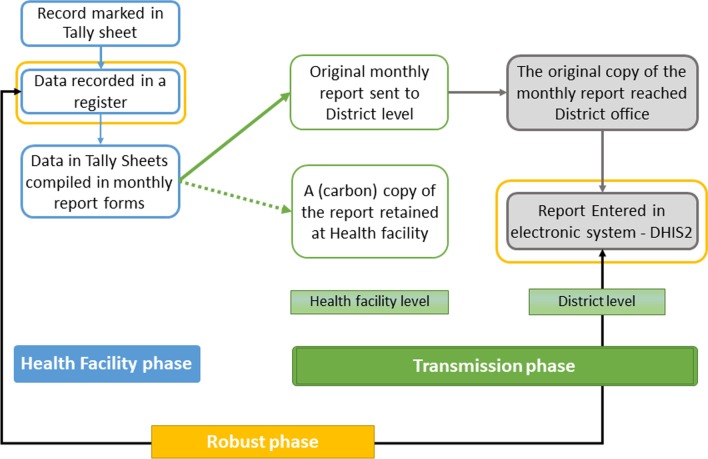
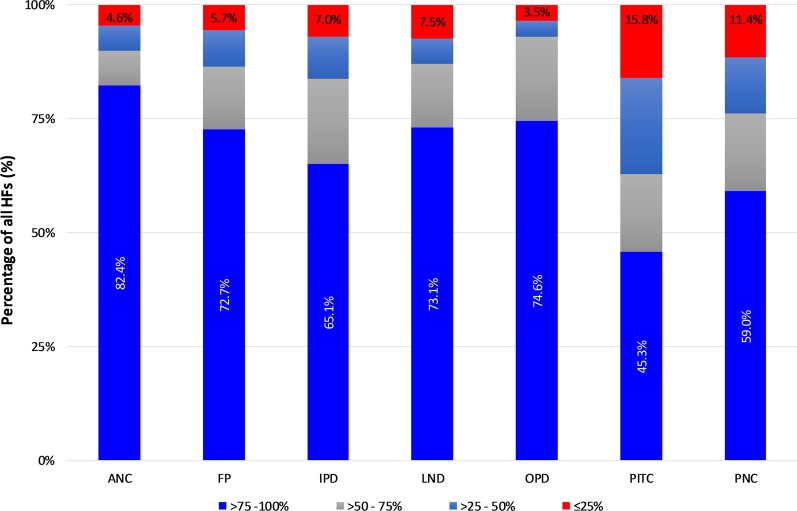
Methods: This cross-sectional study involved reviews of documents, information systems and databases, and collection of primary data from facility-level registers, tally sheets and monthly summary reports. Thirty-four indicators from Outpatient, Inpatient, Antenatal care, Family Planning, Post-natal care, Labour and Delivery, and Provider-Initiated Testing and Counselling service areas were assessed. Indicator records were tracked and compared across the process of data collection, compilation and submission to the district office. Copies of monthly report forms submitted by facilities to the district were also reviewed. The availability and utilization of HMIS tools were assessed, while completeness and data accuracy levels were quantified for each phase of the reporting system.
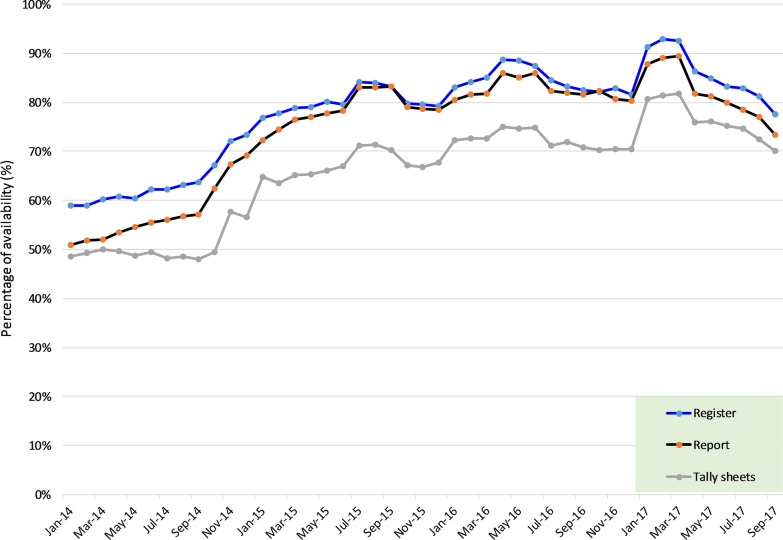
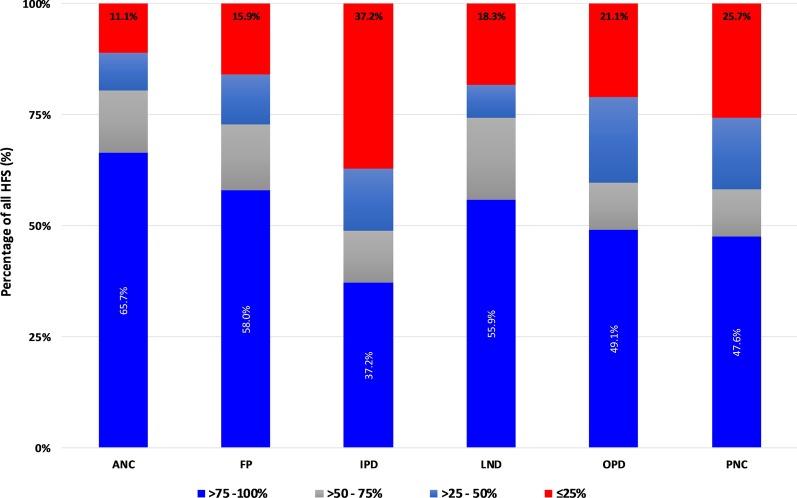
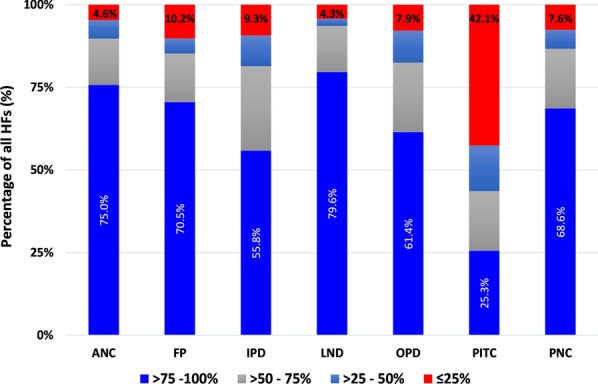
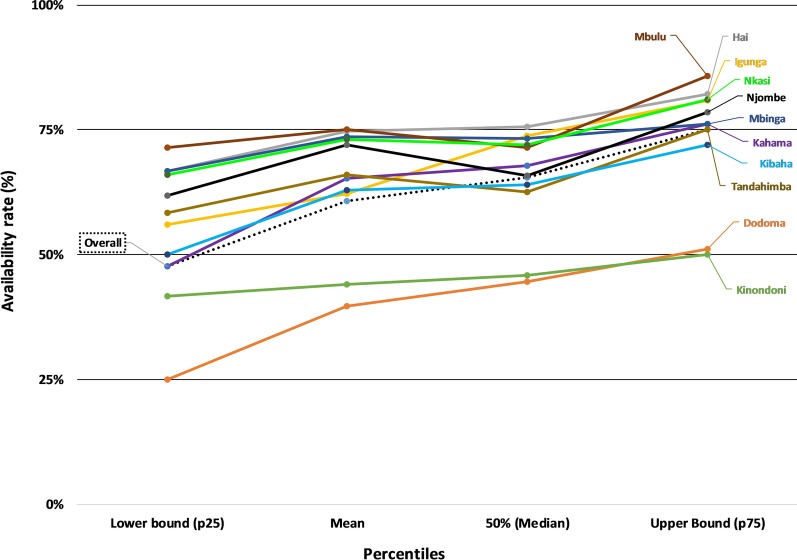
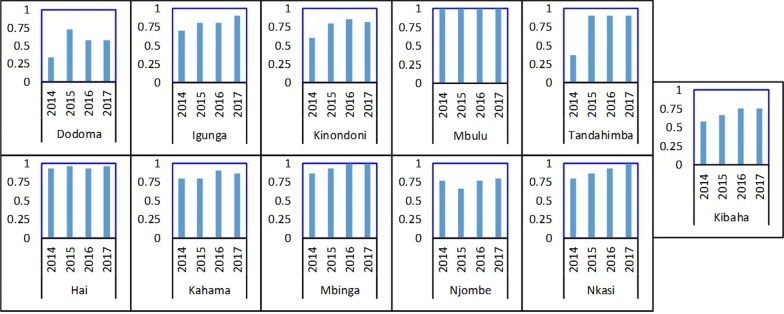
Results: A total of 115 HFs (including hospitals, health centres, dispensaries) in 11 districts were involved. Registers (availability rate = 91.1%; interquartile range (IQR) 66.7-100%) and report forms (86.9%; IQR 62.2-100%) were the most utilized tools. There was a limited use of tally-sheets (77.8%; IQR 35.6-100%). Tools availability at the dispensary was 91.1%, health centre 82.2% and hospital 77.8%, and was low in urban districts. The availability rate at the district level was 65% (IQR 48-75%). Wrongly filled or empty cells in registers and poor adherence to the coding procedures were observed. Reports were highly over-represented in comparison to registers' records, with large differences observed at the HF phase of the reporting system. The OPD and IPD areas indicated the highest levels of mismatch between data source and district office. Indicators with large number of clients, multiple variables, disease categorization, or those linked with dispensing medicine performed poorly.
Conclusion: There are high variations in the tool utilisation and data accuracy at facility and district levels. The routine HMIS is weak and data at district level inaccurately reflects what is available at the source. These results highlight the need to design tailored and inter-service strategies for improving data quality.
Keywords: Accuracy; Completeness; Data; District; Facility; Health information; Indicators; Quality; Tanzania.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Aiga H, Kuroiwa C, Takizawa I, Yamagata R. The reality of health information systems: challenges for standardization. Biosci Trends. 2008;2(1):5–9. - PubMed
-
- Franco L, Fields R, Mmbuji PKL, Posner S, Mboera LEG, Jimmerson A, et al. Situation analysis of infectious disease surveillance in two districts in Tanzania, 2002. Bethesda: Abt Associates Inc.; 2003.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
