

Prognostic Role of Hepatorenal Function Indexes in Patients With Ebstein Anomaly
- PMID: 33334426
- PMCID: PMC7755072
- DOI: 10.1016/j.jacc.2020.10.035
Prognostic Role of Hepatorenal Function Indexes in Patients With Ebstein Anomaly
Abstract
Background: Hepatorenal dysfunction is a risk factor for mortality in patients with chronic tricuspid regurgitation due to acquired heart disease. Ebstein anomaly is the most common cause of primary tricuspid regurgitation in adults with congenital heart disease, but the prevalence and prognostic implications of hepatorenal dysfunction are unknown in this population.
Objectives: The purpose of this study was to determine the risk factors and prognostic implications of hepatorenal dysfunction, as measured primarily by the use of model for end-stage liver disease excluding international normalized ratio (MELD-XI score), as well as looking at other associated factors.
Methods: This was a retrospective study of adults with Ebstein anomaly who received care at Mayo Clinic from 2003 to 2018.
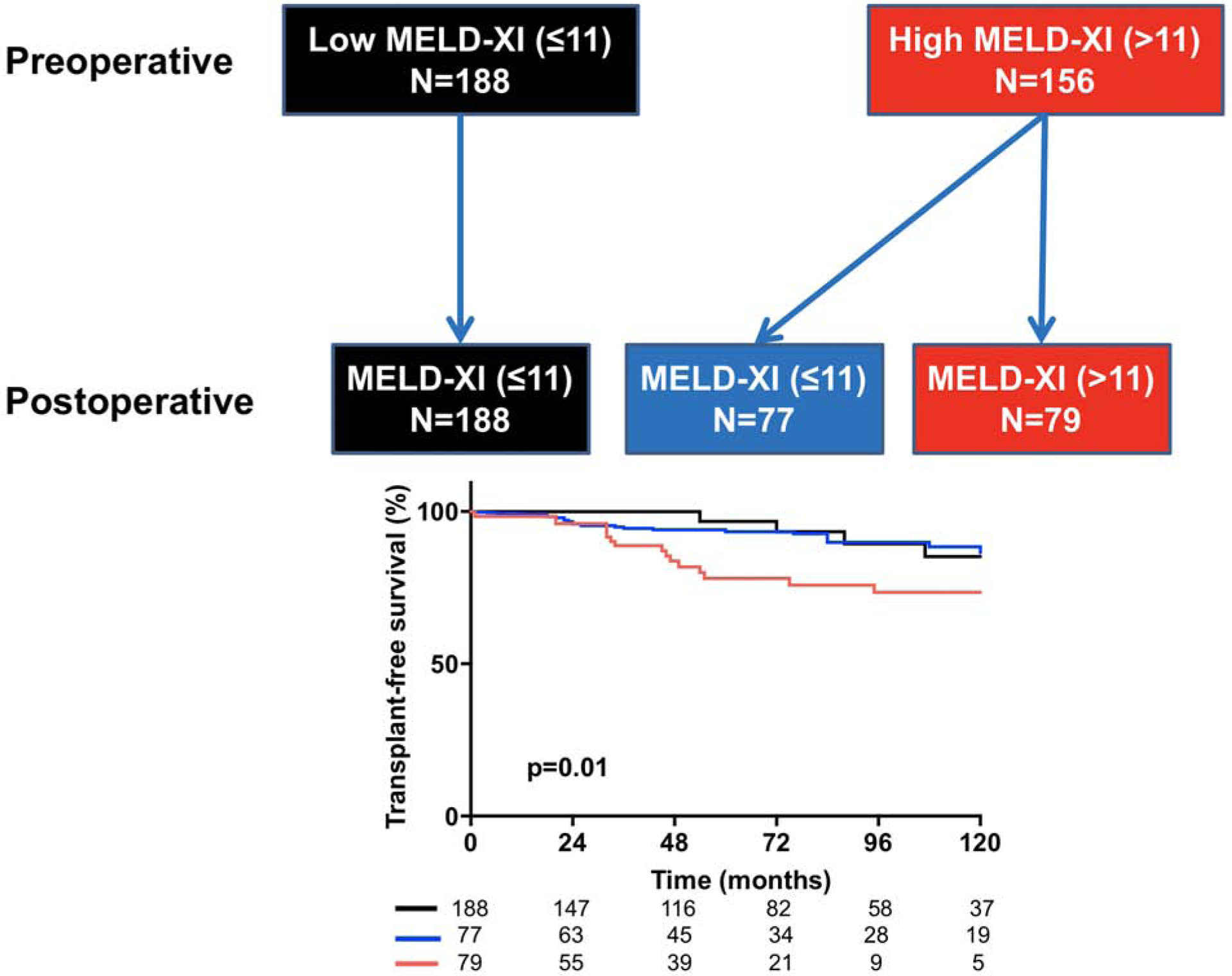
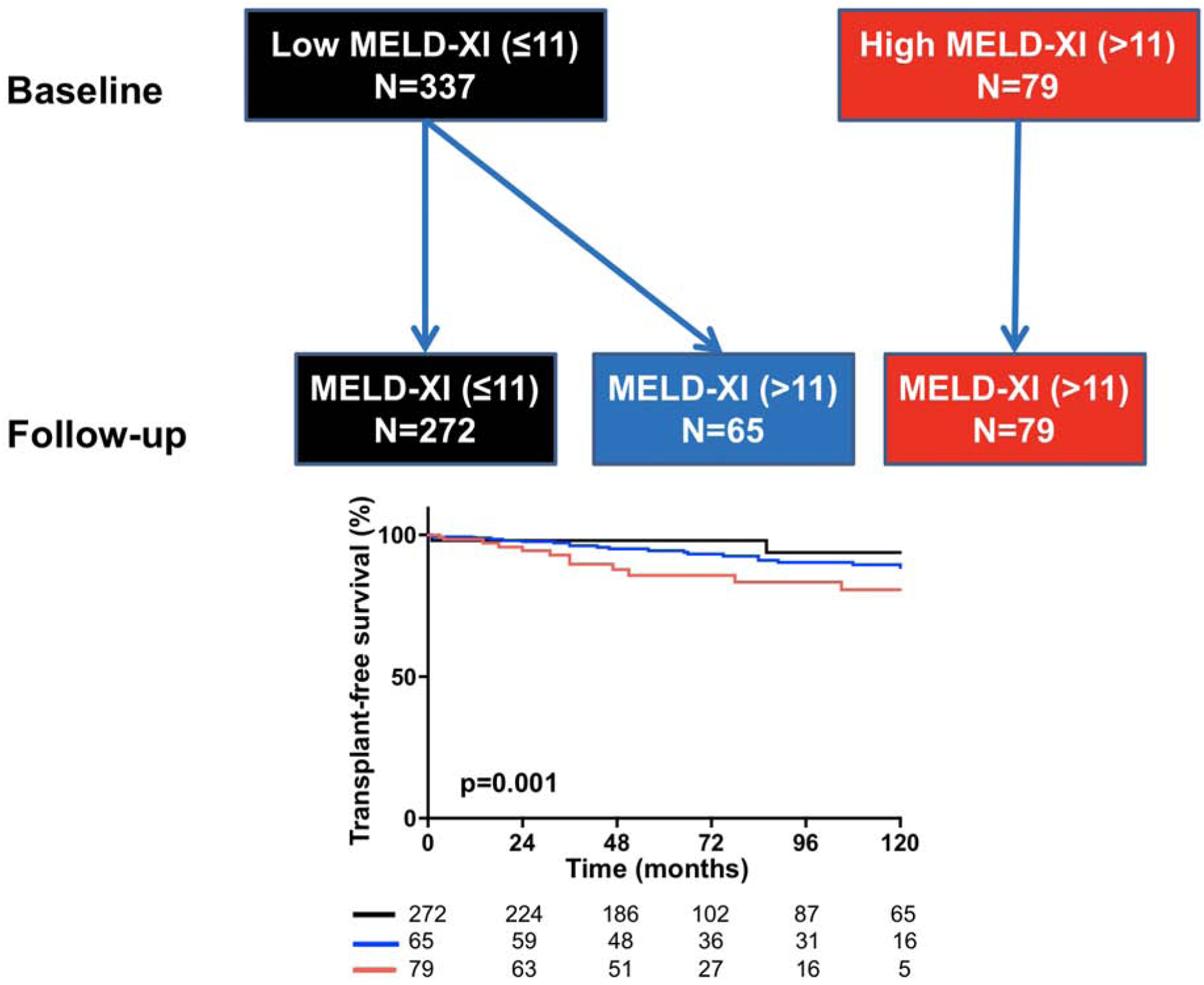
Results: Of 692 patients, the median MELD-XI score was 10.2 (interquartile range: 9.4 to 13.3); 53 (8%) died and 3 (0.4%) underwent heart transplant. MELD-XI was an independent predictor of death/transplant (hazard ratio: 1.32; 95% confidence interval: 1.11 to 2.06; p < 0.001). In the subset of patients with serial MELD-XI scores (n = 416), temporal change in MELD-XI score (ΔMELD-XI) was also a predictor of death/transplant. In the subset of patients who underwent tricuspid valve surgery (n = 344), a post-operative improvement in MELD-XI score (ΔMELD-XI) was associated with improved long-term survival. Impaired right atrial (RA) reservoir strain and elevated estimated RA pressure were associated with worse baseline MELD-XI and ΔMELD-XI scores.
Conclusions: Hepatorenal dysfunction is a predictor of mortality in Ebstein anomaly, and RA dysfunction and hypertension are hemodynamic biomarkers that can identify patients at risk for deterioration in hepatorenal function and mortality. These data highlight the prognostic importance of noncardiac organ-system dysfunction, and provide complementary clinical risk stratification metrics for management of these patients.
Keywords: Ebstein anomaly; hepatorenal dysfunction; mortality.
Copyright © 2020 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Author Disclosures The MACHD Registry is supported by the Al-Bahar Research grant. Dr. Egbe is supported by National Heart, Lung, and Blood Institute grant K23 HL141448. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures
Comment in
-
Risk Assessment in Patients With Tricuspid Valve Regurgitation: MELD and Beyond.J Am Coll Cardiol. 2020 Dec 22;76(25):2977-2979. doi: 10.1016/j.jacc.2020.11.009. Epub 2020 Nov 9. J Am Coll Cardiol. 2020. PMID: 33181244 No abstract available.
References
-
- Xanthopoulos A, Starling RC, Kitai T, Triposkiadis F. Heart Failure and Liver Disease: Cardiohepatic Interactions. JACC Heart Fail. 2019. February;7(2):87–97. - PubMed
-
- Rangaswami J, Bhalla V, Blair JEA, Chang TI, Costa S, Lentine KL, Lerma EV, Mezue K, Molitch M, Mullens W, Ronco C, Tang WHW, McCullough PA; American Heart Association Council on the Kidney in Cardiovascular Disease and Council on Clinical Cardiology. Cardiorenal Syndrome: Classification, Pathophysiology, Diagnosis, and Treatment Strategies: A Scientific Statement From the American Heart Association. Circulation. 2019. April 16;139(16):e840–e878. - PubMed
-
- Maeder MT, Holst DP, Kaye DM. Tricuspid regurgitation contributes to renal dysfunction in patients with heart failure. J Card Fail. 2008. December;14(10):824–30. - PubMed
-
- Aziz TM, Saad RA, Burgess MI, Campbell CS, Yonan NA. Clinical significance of tricuspid valve dysfunction after orthotopic heart transplantation. J Heart Lung Transplant. 2002. October;21(10):1101–8. - PubMed
-
- Lau GT, Tan HC, Kritharides L. Type of liver dysfunction in heart failure and its relation to the severity of tricuspid regurgitation. Am J Cardiol. 2002. December 15;90(12):1405–9. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
