

Puberty Initiates Cascading Relationships Between Neurodevelopmental, Social, and Internalizing Processes Across Adolescence
- PMID: 33334434
- PMCID: PMC8494463
- DOI: 10.1016/j.biopsych.2020.09.002
Puberty Initiates Cascading Relationships Between Neurodevelopmental, Social, and Internalizing Processes Across Adolescence
Abstract
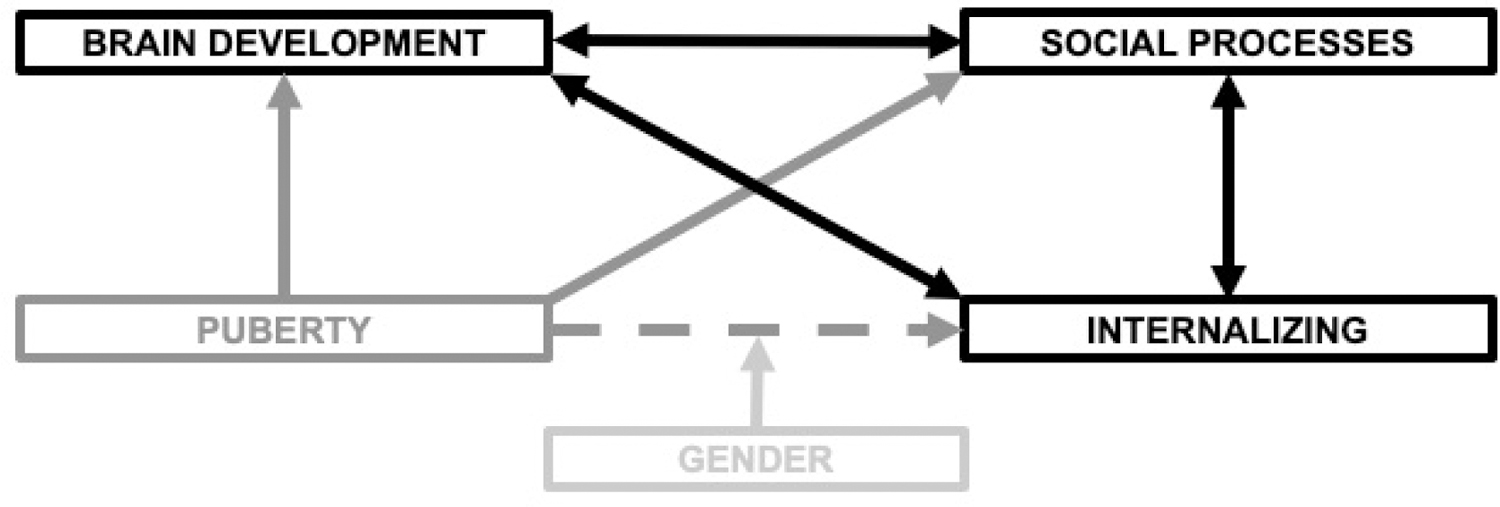
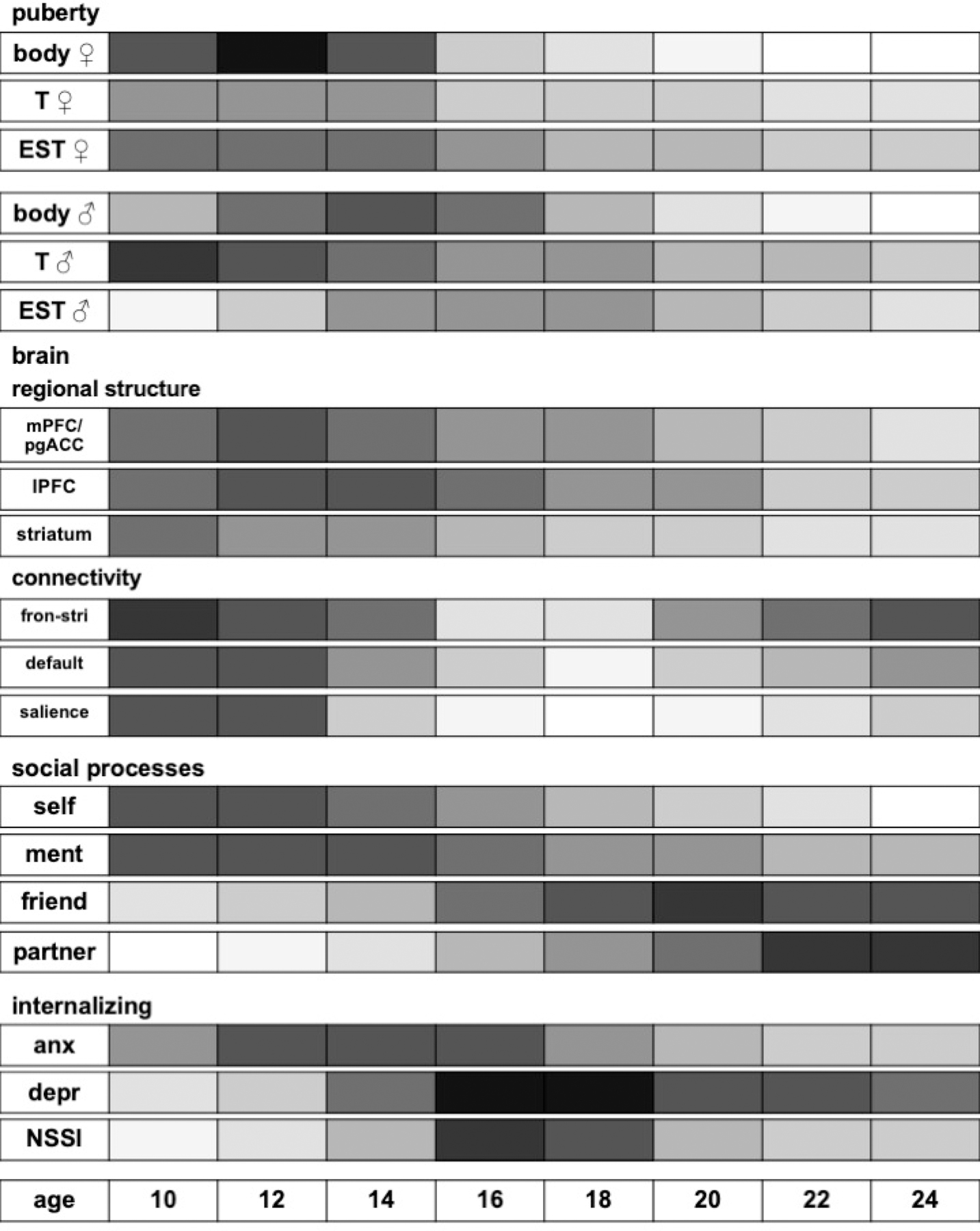
Adolescence is a period of dramatic developmental transitions-from puberty-related changes in hormones, bodies, and brains to an increasingly complex social world. The concurrent increase in the onset of many mental disorders has prompted the search for key developmental processes that drive changes in risk for psychopathology during this period of life. Hormonal surges and consequent physical maturation linked to pubertal development in adolescence are thought to affect multiple aspects of brain development, social cognition, and peer relations, each of which have also demonstrated associations with risk for mood and anxiety disorders. These puberty-related effects may combine with other nonpubertal influences on brain maturation to transform adolescents' social perception and experiences, which in turn continue to shape both mental health and brain development through transactional processes. In this review, we focus on pubertal, neural, and social changes across the duration of adolescence that are known or thought to be related to adolescent-emergent disorders, specifically depression, anxiety, and deliberate self-harm (nonsuicidal self-injury). We propose a theoretical model in which social processes (both social cognition and peer relations) are critical to understanding the way in which pubertal development drives neural and psychological changes that produce potential mental health vulnerabilities, particularly (but not exclusively) in adolescent girls.
Keywords: Internalizing; Neurodevelopment; Puberty; Social cognition; Social connection; Social rejection.
Copyright © 2020 Society of Biological Psychiatry. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Financial Disclosures
Dr. Pfeifer reports no biomedical financial interests or potential conflicts of interest. Dr. Allen has an equity interest in Ksana Health, Inc., for which he is the co-founder and CEO.
Figures
References
-
- Hankin BL, Abramson LY, Moffitt TE, Silva PA, McGee R, Angell KE (1998): Development of depression from preadolescence to young adulthood: emerging gender differences in a 10-year longitudinal study. J Abnorm Psychol 107: 128–140. - PubMed
-
- Hyde JS, Mezulis AH, Abramson LY (2008): The ABCs of depression: Integrating affective, biological, and cognitive models to explain the emergence of the gender difference in depression. Psychological Review 115: 291–313. - PubMed
-
- Nolen-Hoeksema S (2001): Gender Differences in Depression. Curr Dir Psychol Sci 10: 173–176.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
