

Spinal CSF-Venous Fistulas in Morbidly and Super Obese Patients with Spontaneous Intracranial Hypotension
- PMID: 33334852
- PMCID: PMC7872193
- DOI: 10.3174/ajnr.A6895
Spinal CSF-Venous Fistulas in Morbidly and Super Obese Patients with Spontaneous Intracranial Hypotension
Abstract
Background and purpose: Spinal CSF-venous fistulas are increasingly recognized as the cause of spontaneous intracranial hypotension. Here, we describe the challenges in the care of patients with CSF-venous fistulas who are morbidly or super obese.
Materials and methods: A review was undertaken of all patients with spontaneous intracranial hypotension and a body mass index of >40 who underwent digital subtraction myelography in the lateral decubitus position to look for CSF-venous fistulas.
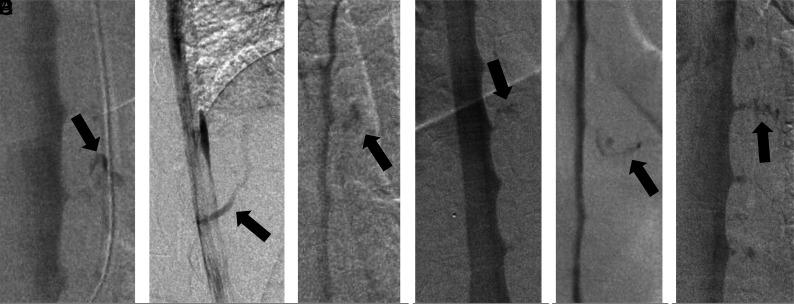
Results: Eight patients with spontaneous intracranial hypotension with a body mass index of >40 underwent lateral decubitus digital subtraction myelography. The mean age of these 5 women and 3 men was 53 years (range, 45 to 68 years). Six patients were morbidly obese (body mass indexes = 40.2, 40.6, 41, 41.8, 45.4, and 46.9), and 2 were super obese (body mass indexes = 53.7 and 56.3). Lumbar puncture showed an elevated opening pressure in 5 patients (26.5-47 cm H2O). The combination of an elevated opening pressure and normal conventional spine imaging findings resulted in a misdiagnosis (midbrain glioma and demyelinating disease, respectively) in 2 patients. Prior treatment included surgical nerve root ligation for suspected CSF-venous fistula in 3 patients. Digital subtraction myelography demonstrated a CSF-venous fistula in 6 patients (75%). Rebound high-pressure headache occurred in all 6 patients following surgical ligation of the fistula, and papilledema developed in 3.
Conclusions: In our series, opening pressure was generally elevated in patients with morbid or super obesity. The yield of identifying CSF-venous fistulas with digital subtraction myelography in this patient population can approach that of the nonobese patient population. These patients may be at higher risk of developing rebound high-pressure headaches and papilledema.
© 2021 by American Journal of Neuroradiology.
Figures

References
-
- Robblee J, Secora KA, Alhilali LM, et al. Spontaneous intracranial hypotension. Pract Neurol 2020. https://practicalneurology.com/articles/2020-may/spontaneous-intracrania.... Accessed August 1, 2020
MeSH terms
LinkOut - more resources
Full Text Sources