

Non-EPI versus Multishot EPI DWI in Cholesteatoma Detection: Correlation with Operative Findings
- PMID: 33334855
- PMCID: PMC7959419
- DOI: 10.3174/ajnr.A6911
Non-EPI versus Multishot EPI DWI in Cholesteatoma Detection: Correlation with Operative Findings
Abstract
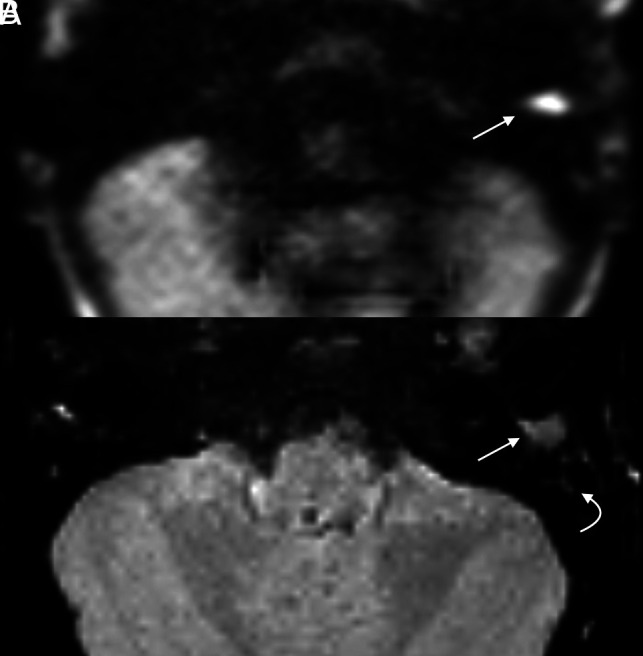
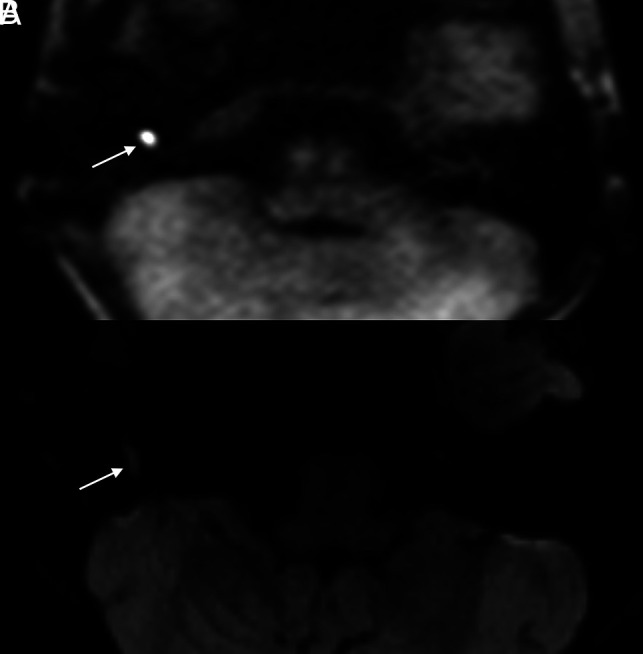
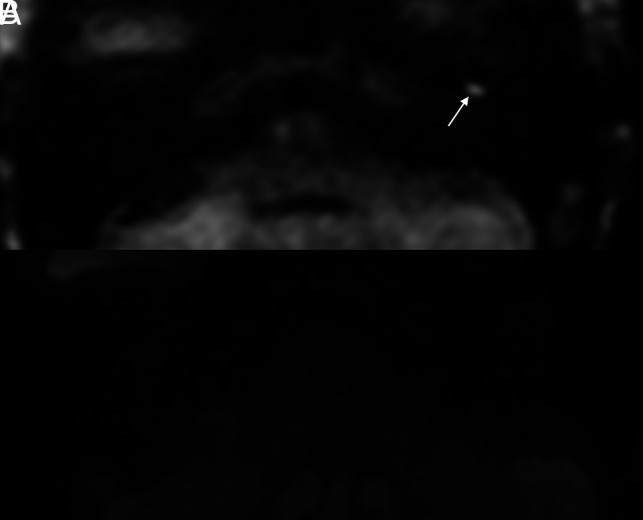
Background and purpose: Although multishot EPI (readout-segmented EPI) has been touted as a robust DWI sequence for cholesteatoma evaluation, its efficacy in disease detection compared with a non-EPI (eg, HASTE) technique is unknown. This study sought to compare the accuracy of readout-segmented EPI with that of HASTE DWI in cholesteatoma detection.
Materials and methods: A retrospective review was completed of consecutive patients who underwent MR imaging for the evaluation of suspected primary or recurrent/residual cholesteatomas. Included patients had MR imaging examinations that included both HASTE and readout-segmented EPI sequences and confirmed cholesteatomas on a subsequent operation. Two neuroradiologist reviewers assessed all images, with discrepancies resolved by consensus. The ratio of signal intensity between the cerebellum and any observed lesion was noted.
Results: Of 23 included patients, 12 (52.2%) were women (average age, 47.8 [SD, 25.2] years). All patients had surgically confirmed cholesteatomas: Six (26.1%) were primary and 17 (73.9%) were recidivistic. HASTE images correctly identified cholesteatomas in 100.0% of patients. On readout-segmented EPI sequences, 16 (69.6%) were positive, 5 (21.7%) were equivocal, and 2 (8.7%) were falsely negative. Excellent interobserver agreement was noted between reviews on both HASTE (κ = 1.0) and readout-segmented EPI (κ = 0.9) sequences. The average signal intensity ratio was significantly higher on HASTE than in readout-segmented EPI, facilitating enhanced detection (mean difference 0.5; 95% CI, 0.3-0.8; P = .003).
Conclusions: HASTE outperforms readout-segmented EPI in the detection of primary cholesteatoma and disease recidivism.
© 2021 by American Journal of Neuroradiology.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources