

Targeted proteomics of right heart adaptation to pulmonary arterial hypertension
- PMID: 33334941
- PMCID: PMC8029214
- DOI: 10.1183/13993003.02428-2020
Targeted proteomics of right heart adaptation to pulmonary arterial hypertension
Abstract
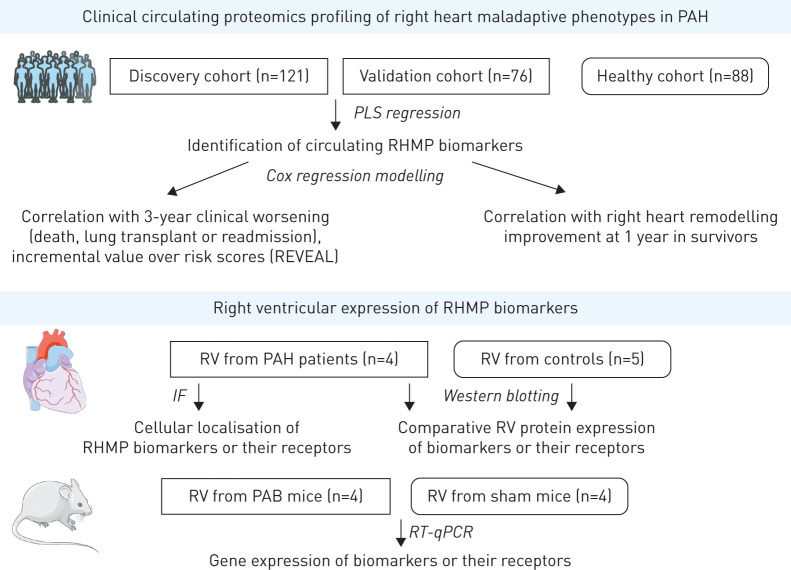
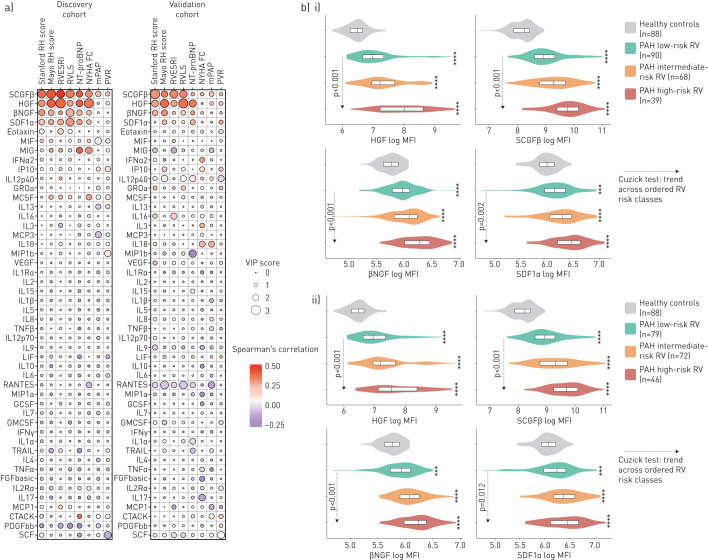
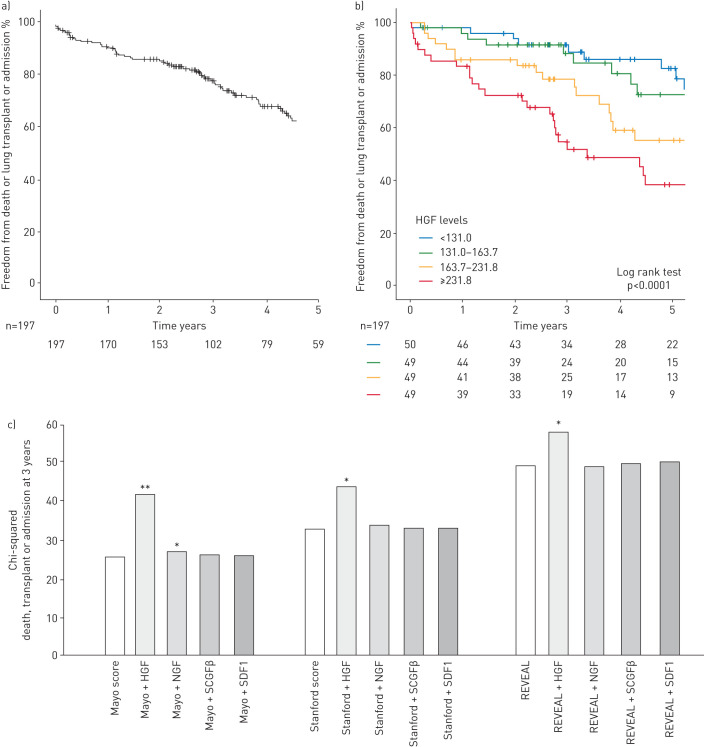
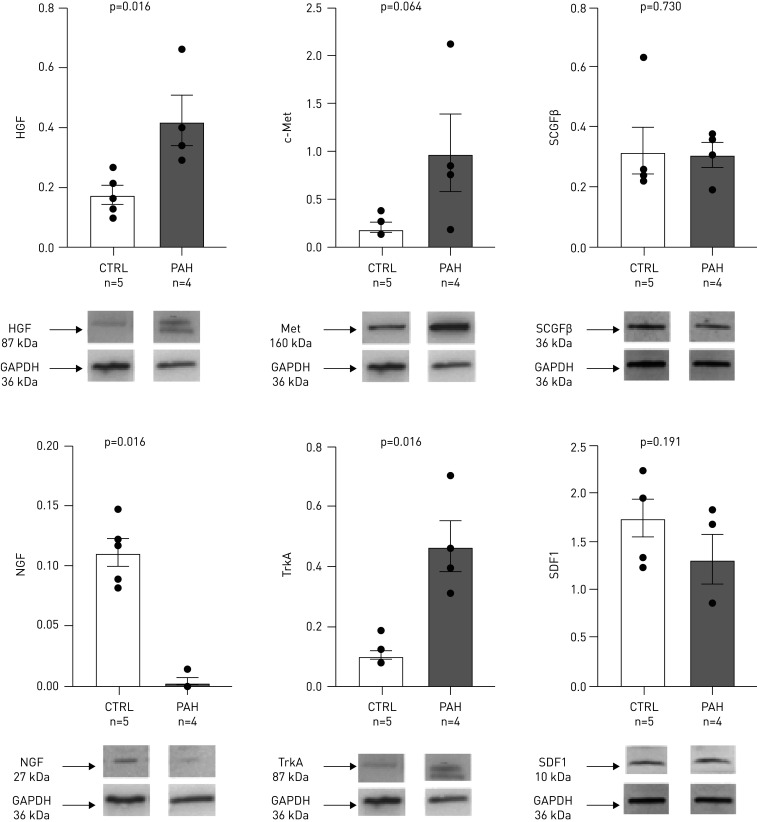
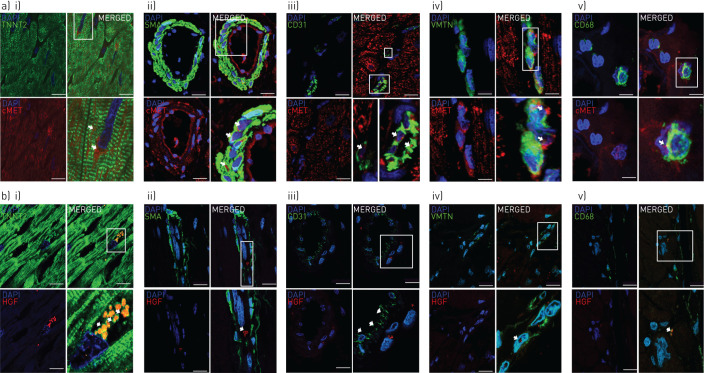
No prior proteomic screening study has centred on the right ventricle (RV) in pulmonary arterial hypertension (PAH). This study investigates the circulating proteomic profile associated with right heart maladaptive phenotype (RHMP) in PAH.Plasma proteomic profiling was performed using multiplex immunoassay in 121 (discovery cohort) and 76 (validation cohort) PAH patients. The association between proteomic markers and RHMP, defined by the Mayo right heart score (combining RV strain, New York Heart Association (NYHA) class and N-terminal pro-brain natriuretic peptide (NT-proBNP)) and Stanford score (RV end-systolic remodelling index, NYHA class and NT-proBNP), was assessed by partial least squares regression. Biomarker expression was measured in RV samples from PAH patients and controls, and pulmonary artery banding (PAB) mice.High levels of hepatocyte growth factor (HGF), stem cell growth factor-β, nerve growth factor and stromal derived factor-1 were associated with worse Mayo and Stanford scores independently from pulmonary resistance or pressure in both cohorts (the validation cohort had more severe disease features: lower cardiac index and higher NT-proBNP). In both cohorts, HGF added value to the REVEAL score in the prediction of death, transplant or hospitalisation at 3 years. RV expression levels of HGF and its receptor c-Met were higher in end-stage PAH patients than controls, and in PAB mice than shams.High plasma HGF levels are associated with RHMP and predictive of 3-year clinical worsening. Both HGF and c-Met RV expression levels are increased in PAH. Assessing plasma HGF levels might identify patients at risk of heart failure who warrant closer follow-up and intensified therapy.
Copyright ©ERS 2021.
Conflict of interest statement
Conflict of interest: M. Amsallem has received a 2016 Young Investigator Seed Grant from the Vera Moulton Wall Center at Stanford, a 2019–2020 Stanford Maternal and Child Health Research Institute research seed grant, a research grant from Actelion-Janssen and speaker fees from Bayer. Conflict of interest: A.J. Sweatt has nothing to disclose. Conflict of interest: J. Arthur Ataam has nothing to disclose. Conflict of interest: J. Guihaire has nothing to disclose. Conflict of interest: F. Lecerf has nothing to disclose. Conflict of interest: M. Lambert has nothing to disclose. Conflict of interest: M.R. Ghigna has nothing to disclose. Conflict of interest: M.K. Ali has nothing to disclose. Conflict of interest: Y. Mao has nothing to disclose. Conflict of interest: E. Fadel has nothing to disclose. Conflict of interest: M. Rabinovitch has nothing to disclose. Conflict of interest: V. de Jesus Perez has nothing to disclose. Conflict of interest: E. Spiekerkoetter is funded by Stanford Cardiovascular Institute, National Heart Lung Blood Institute (NHLBI) at the National Institute of Health (NIH) grant R01 HL128734 and Department of Defense grant PR161256. Conflict of interest: O. Mercier has been supported by a public grant overseen by the French National Research Agency as part of the second Investissement d'Avenir program (ANR-15-RHUS-0002). Conflict of interest: F. Haddad has received research grants from Actelion-Janssen and Philips. Conflict of interest: R.T. Zamanian has nothing to disclose.
Figures
Comment in
-
Utilising biomarkers to predict right heart maladaptive phenotype: a step toward precision medicine.Eur Respir J. 2021 Apr 8;57(4):2004506. doi: 10.1183/13993003.04506-2020. Print 2021 Apr. Eur Respir J. 2021. PMID: 33833075 No abstract available.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous