

Impact of intraoperative margin clearance on survival following pancreatoduodenectomy for pancreatic cancer: a systematic review and meta-analysis
- PMID: 33335201
- PMCID: PMC7746710
- DOI: 10.1038/s41598-020-79252-8
Impact of intraoperative margin clearance on survival following pancreatoduodenectomy for pancreatic cancer: a systematic review and meta-analysis
Abstract
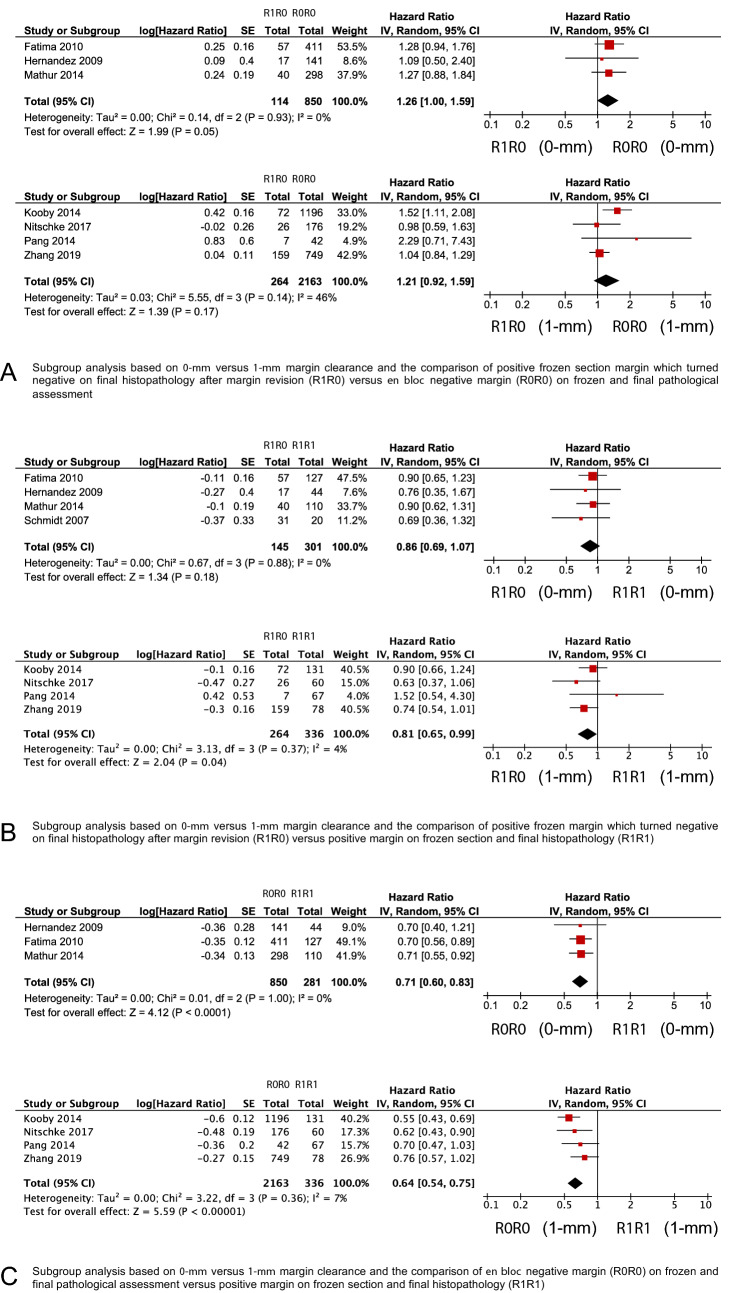
The use of intraoperative margin revision to achieve margin clearance in patients undergoing pancreatoduodenectomy for pancreatic cancer is controversial. We performed a systematic review and meta-analysis to summarize the evidence of intraoperative margin revisions of the pancreatic neck and its impact on overall survival (OS). Nine studies with 4501 patients were included. Patient cohort was stratified in an R0R0-group (negative margin on frozen and permanent section), R1R0-group (revised positive margin on frozen section which turned negative on permanent section), and R1R1-group (positive margin on frozen and permanent section despite margin revision). OS was higher in the R1R0-group (HR 0.83, 95% CI 0.72-0.96, P = 0.01) compared to the R1R1-group but lower compared to the R0R0-group (HR 1.20; 95% CI 1.05-1.37, P = 0.008), respectively. Subgroup analyses on the use of different margin clearance definitions confirmed an OS benefit in the R1R0-group compared to the R1R1-group (HR 0.81; 95% CI 0.65-0.99, P = 0.04). In conclusion, intraoperative margin clearance of the pancreatic neck margin is associated with improved OS while residual tumor indicates aggressive tumor biology. Consensus definitions on margin terminologies, clearance, and surgical techniques are required.
Conflict of interest statement
The authors declare no competing interests.
Figures


References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
