

Modified hemispherectomy for infantile hemiparesis and epilepsy
- PMID: 33335778
- PMCID: PMC7718624
- DOI: 10.1515/tnsci-2020-0145
Modified hemispherectomy for infantile hemiparesis and epilepsy
Abstract
Objective: To investigate the effect and medical imaging of modified hemispherectomy on patients with infantile hemiparesis and medically refractory epilepsy.
Patients and methods: Forty-three patients with infantile hemiparesis and refractory epilepsy who underwent hemispherectomy were enrolled. The treatment effect and medical imaging were analyzed.
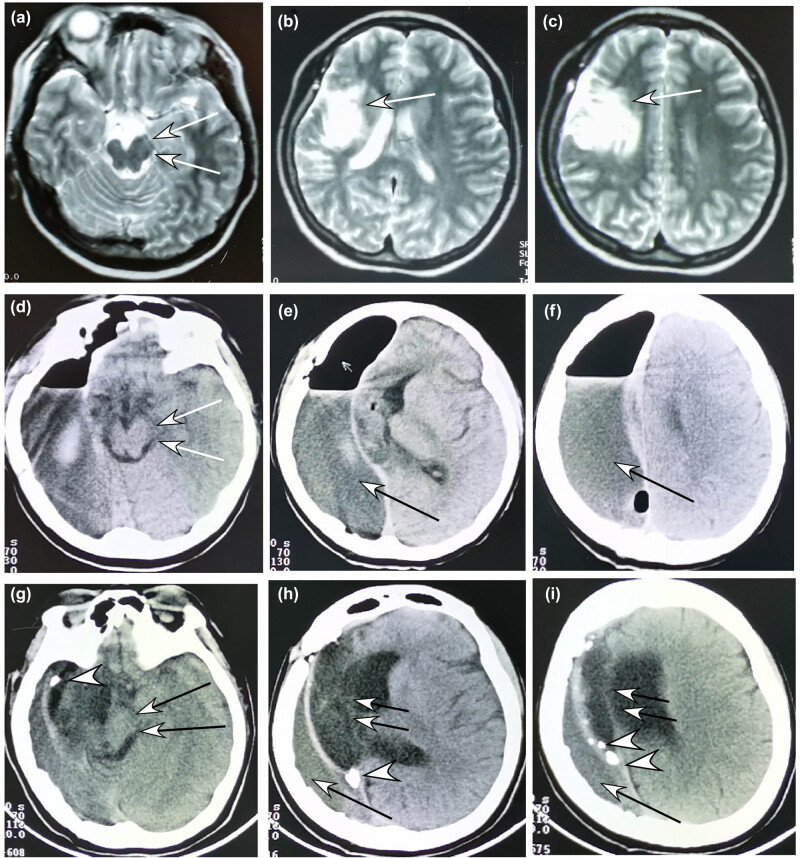
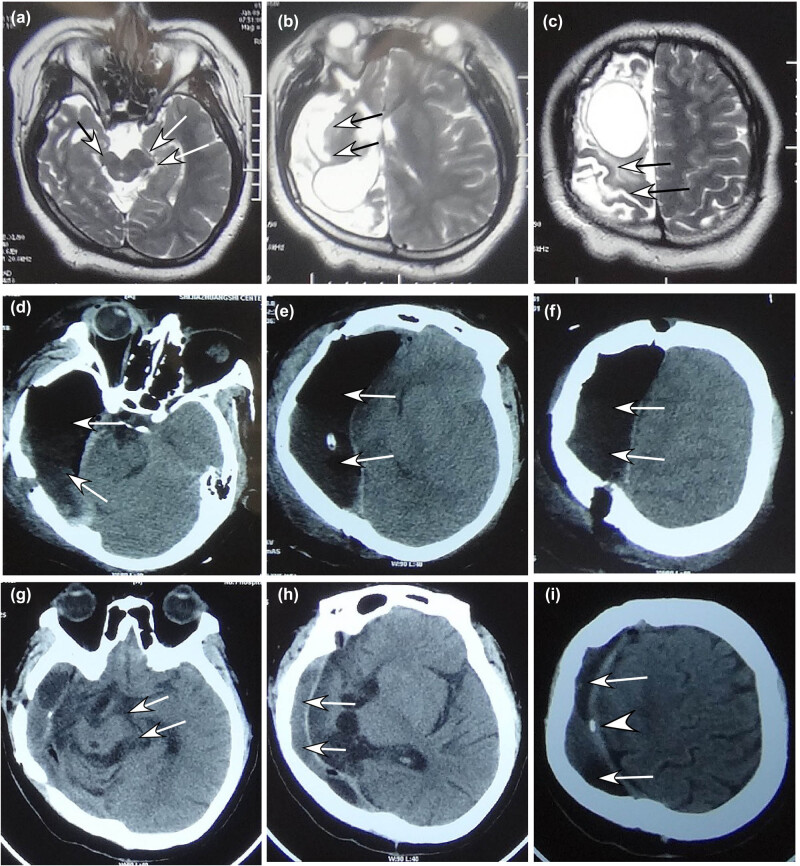
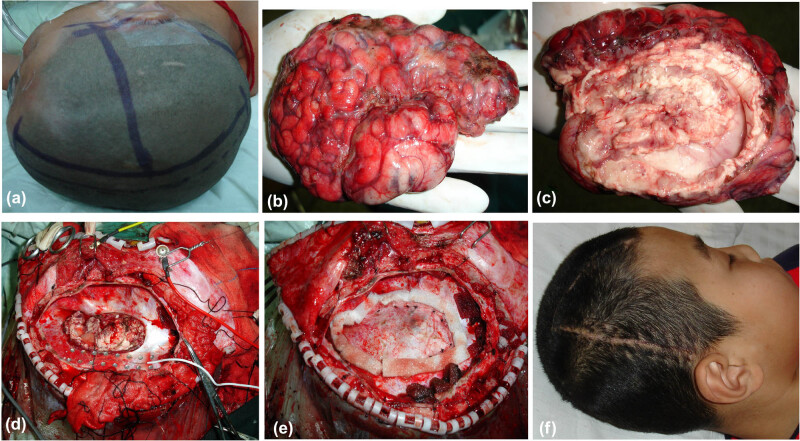
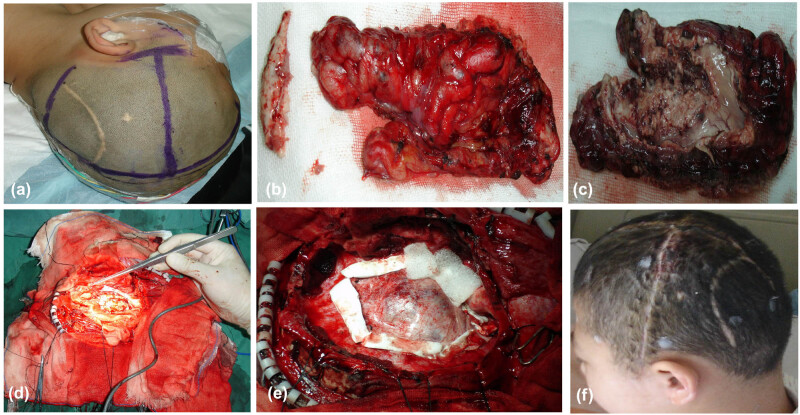
Results: Anatomical hemispherectomy was successfully performed in all patients (100%). In all patients, the muscular tension decreased and the contracted limbs relaxed. In the pathological examination of the resected brain tissue, secondary cicatricial gyri with concomitant cortical dysplasia was present in 36 cases and polycerebellar gyrus malformation and porencephalia in the other 7 cases. Followed up for 7-15 years (mean 11.3), all patients were alive without a long-term sequela. Epilepsy was satisfactorily controlled, with complete seizure relief in 39 cases (91%) classified as Engel I and basic control in the other 4 (9%) defined as Engel II. The posthemispherectomy medical imaging demonstrated that the intracranial space on the operative side shrank, and the healthy cerebral hemisphere shifted markedly toward the hemispherectomy side, with expanded lateral ventricle on the healthy side and thickened skull and enlarged frontal sinus on the operative side. After 4-5 years, the intracranial space on the operative side disappeared in 75% of the patients, demonstrating enlarged cerebral peduncle on the healthy side.
Conclusion: Further modified hemispherectomy in patients with infantile hemiparesis and medically refractory epilepsy demonstrated markedly ameliorated effects on epilepsy control and the prevention of superficial cerebral hemosiderosis in the long-term follow-up.
Keywords: complications; hemispherectomy; infantile hemiparesis; medical imaging; refractory epilepsy.
© 2020 Yu-Hui Li et al., published by De Gruyter.
Conflict of interest statement
Conflict of interest: The authors state no conflicts of interest.
Figures

Similar articles
-
[Pathologic features of ulegyria in refractory epilepsy by modified anatomic hemispherectomy: a clinicopathologic study of 39 cases].Zhonghua Bing Li Xue Za Zhi. 2012 Oct;41(10):671-5. doi: 10.3760/cma.j.issn.0529-5807.2012.10.006. Zhonghua Bing Li Xue Za Zhi. 2012. PMID: 23302308 Chinese.
-
[Modified hemispherectomy for intractable epilepsy in patients with infantile hemiplegia].Zhonghua Wai Ke Za Zhi. 2005 Nov 1;43(21):1410-3. Zhonghua Wai Ke Za Zhi. 2005. PMID: 16318783 Chinese.
-
Symptomatic epilepsy in children with poroencephalic cysts secondary to perinatal middle cerebral artery occlusion.Childs Nerv Syst. 2006 Aug;22(8):922-30. doi: 10.1007/s00381-006-0150-3. Epub 2006 Jul 1. Childs Nerv Syst. 2006. PMID: 16816980 Clinical Trial.
-
Outcomes after hemispherectomy in adult patients with intractable epilepsy: institutional experience and systematic review of the literature.J Neurosurg. 2018 Mar;128(3):853-861. doi: 10.3171/2016.9.JNS151778. Epub 2017 Apr 28. J Neurosurg. 2018. PMID: 28452614
-
Current management and surgical outcomes of medically intractable epilepsy.Clin Neurol Neurosurg. 2013 Dec;115(12):2411-8. doi: 10.1016/j.clineuro.2013.09.035. Epub 2013 Oct 11. Clin Neurol Neurosurg. 2013. PMID: 24169149 Review.
References
-
- Bahuleyan B, Robinson S, Nair AR, Sivanandapanicker JL, Cohen AR. Anatomic hemispherectomy: historical perspective. World Neurosurg. 2013;80:396–8. - PubMed
- Bahuleyan B, Robinson S, Nair AR, Sivanandapanicker JL, Cohen AR. Anatomic hemispherectomy: historical perspective. World Neurosurg. 2013;80:396–8. - PubMed
-
- Holloway V, Gadian DG, Vargha-Khadem F, Porter DA, Boyd SG, Connelly A. The reorganization of sensorimotor function in children after hemispherectomy. A functional MRI and somatosensory evoked potential study. Brain. 2000;123(Pt 12):2432–44. - PubMed
- Holloway V, Gadian DG, Vargha-Khadem F, Porter DA, Boyd SG, Connelly A. The reorganization of sensorimotor function in children after hemispherectomy. A functional MRI and somatosensory evoked potential study. Brain. 2000;123(Pt 12):2432–44. - PubMed
-
- Lin Y, Harris DA, Curry DJ, Lam S. Trends in outcomes, complications, and hospitalization costs for hemispherectomy in the united states for the years 2000–2009. Epilepsia. 2015;56:139–46. - PubMed
- Lin Y, Harris DA, Curry DJ, Lam S. Trends in outcomes, complications, and hospitalization costs for hemispherectomy in the united states for the years 2000–2009. Epilepsia. 2015;56:139–46. - PubMed
-
- Baumgartner JE, Blount JP, Blauwblomme T, Chandra PS. Technical descriptions of four hemispherectomy approaches: from the pediatric epilepsy surgery meeting at gothenburg 2014. Epilepsia. 2017;58(Suppl 1):46–55. - PubMed
- Baumgartner JE, Blount JP, Blauwblomme T, Chandra PS. Technical descriptions of four hemispherectomy approaches: from the pediatric epilepsy surgery meeting at gothenburg 2014. Epilepsia. 2017;58(Suppl 1):46–55. - PubMed
LinkOut - more resources
Full Text Sources