

Challenges and strategies for in situ endothelialization and long-term lumen patency of vascular grafts
- PMID: 33336112
- PMCID: PMC7721596
- DOI: 10.1016/j.bioactmat.2020.11.028
Challenges and strategies for in situ endothelialization and long-term lumen patency of vascular grafts
Abstract
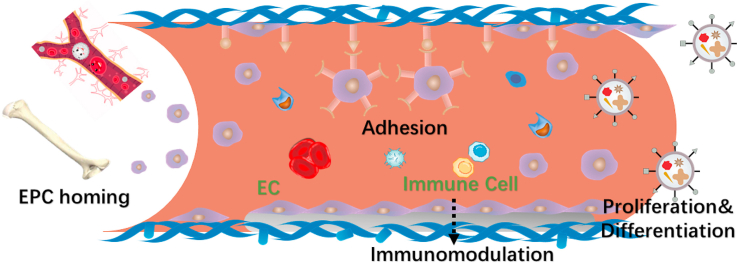
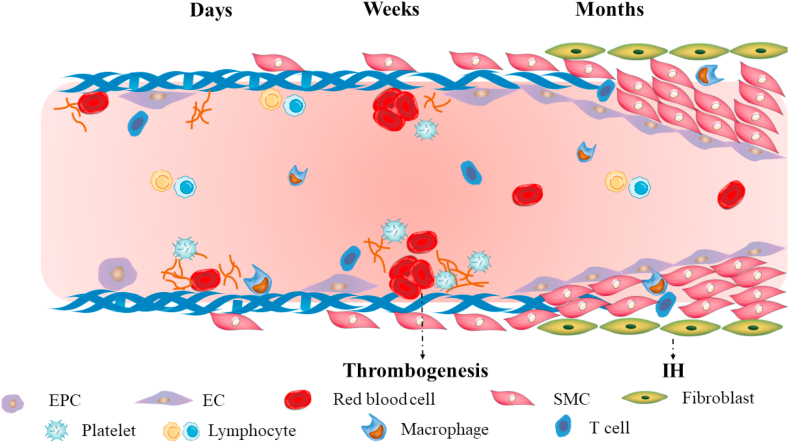
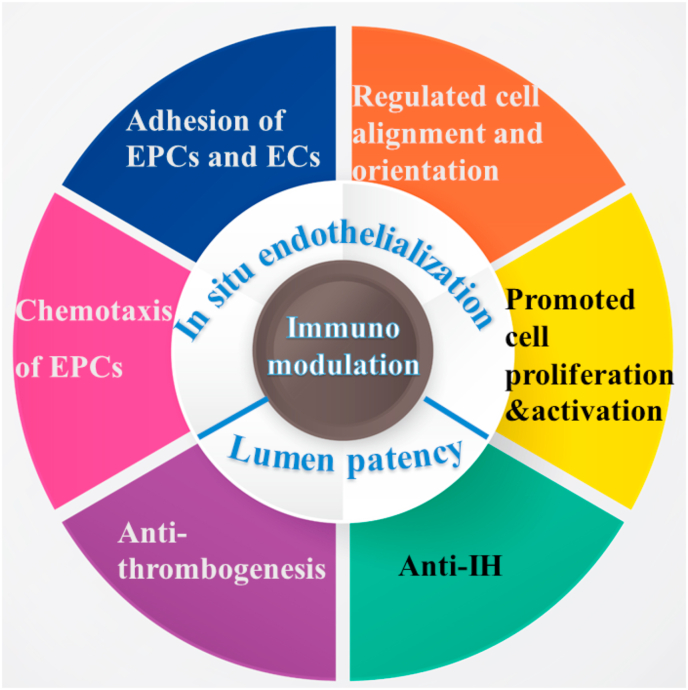
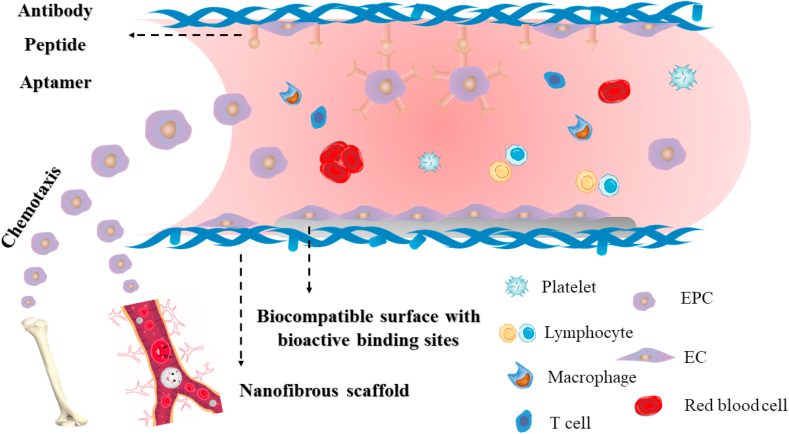
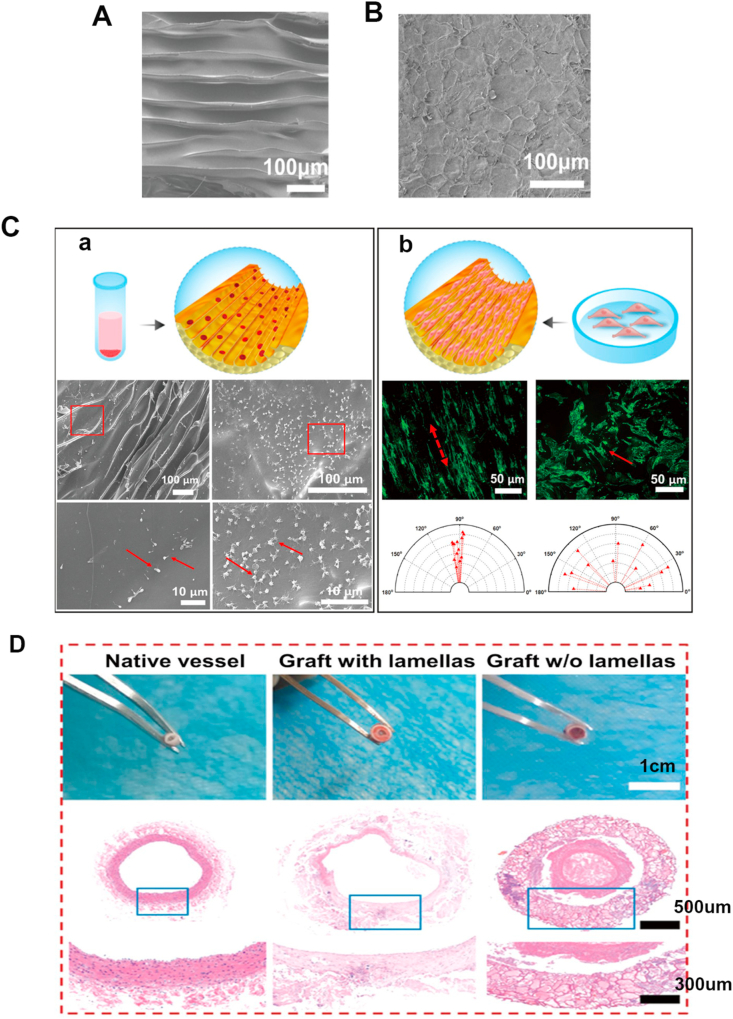
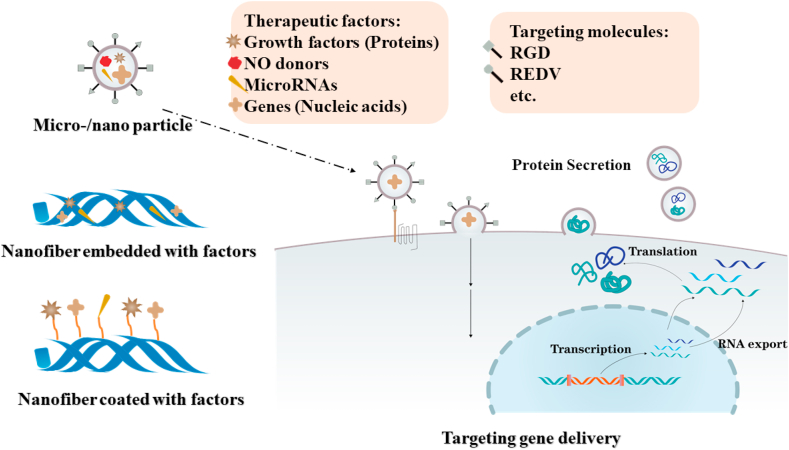
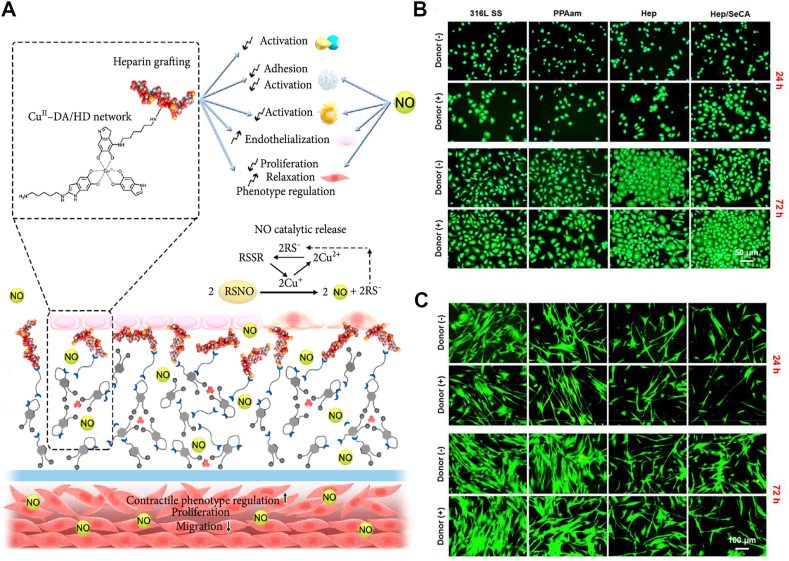
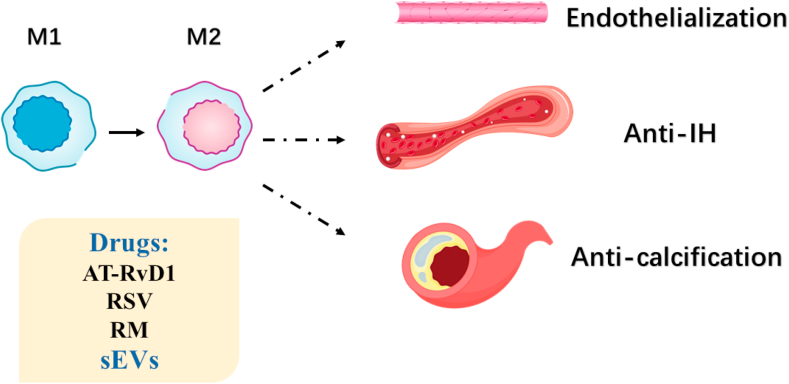
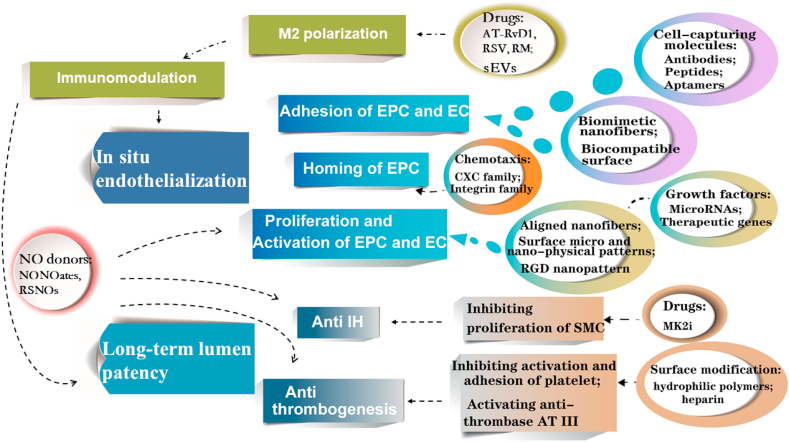
Vascular diseases are the most prevalent cause of ischemic necrosis of tissue and organ, which even result in dysfunction and death. Vascular regeneration or artificial vascular graft, as the conventional treatment modality, has received keen attentions. However, small-diameter (diameter < 4 mm) vascular grafts have a high risk of thrombosis and intimal hyperplasia (IH), which makes long-term lumen patency challengeable. Endothelial cells (ECs) form the inner endothelium layer, and are crucial for anti-coagulation and thrombogenesis. Thus, promoting in situ endothelialization in vascular graft remodeling takes top priority, which requires recruitment of endothelia progenitor cells (EPCs), migration, adhesion, proliferation and activation of EPCs and ECs. Chemotaxis aimed at ligands on EPC surface can be utilized for EPC homing, while nanofibrous structure, biocompatible surface and cell-capturing molecules on graft surface can be applied for cell adhesion. Moreover, cell orientation can be regulated by topography of scaffold, and cell bioactivity can be modulated by growth factors and therapeutic genes. Additionally, surface modification can also reduce thrombogenesis, and some drug release can inhibit IH. Considering the influence of macrophages on ECs and smooth muscle cells (SMCs), scaffolds loaded with drugs that can promote M2 polarization are alternative strategies. In conclusion, the advanced strategies for enhanced long-term lumen patency of vascular grafts are summarized in this review. Strategies for recruitment of EPCs, adhesion, proliferation and activation of EPCs and ECs, anti-thrombogenesis, anti-IH, and immunomodulation are discussed. Ideal vascular grafts with appropriate surface modification, loading and fabrication strategies are required in further studies.
Keywords: Immunomodulation; In situ endothelialization; Intimal hyperplasia; Thrombogenesis; Vascular graft.
© 2020 The Authors. Production and hosting by Elsevier B.V. on behalf of KeAi Communications Co., Ltd.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
References
-
- Roger V.L., Go A.S., Lloyd-Jones D.M., Adams R.J., Berry J.D., Brown T.M., Carnethon M.R., Dai S., de Simone G., Ford E.S., Fox C.S., Fullerton H.J., Gillespie C., Greenlund K.J., Hailpern S.M., Heit J.A., Ho P.M., Howard V.J., Kissela B.M., Kittner S.J., Lackland D.T., Lichtman J.H., Lisabeth L.D., Makuc D.M., Marcus G.M., Marelli A., Matchar D.B., McDermott M.M., Meigs J.B., Moy C.S., Mozaffarian D., Mussolino M.E., Nichol G., Paynter N.P., Rosamond W.D., Sorlie P.D., Stafford R.S., Turan T.N., Turner M.B., Wong N.D., Wylie-Rosett J. Heart disease and stroke statistics--2011 update: a report from the American Heart Association. Circulation. 2011;123(4):e18–e209. doi: 10.1161/CIR.0b013e3182009701. - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
