

Comparative effects of flow vs. volume-controlled one-lung ventilation on gas exchange and respiratory system mechanics in pigs
- PMID: 33336305
- PMCID: PMC7746431
- DOI: 10.1186/s40635-020-00308-0
Comparative effects of flow vs. volume-controlled one-lung ventilation on gas exchange and respiratory system mechanics in pigs
Abstract
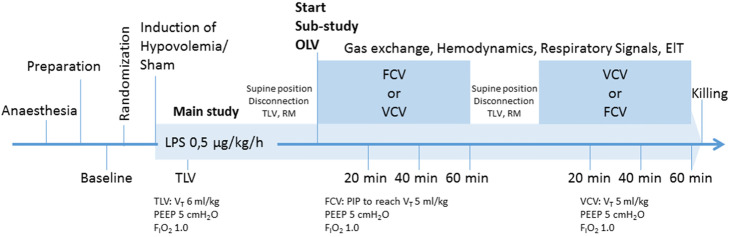
Background: Flow-controlled ventilation (FCV) allows expiratory flow control, reducing the collapse of the airways during expiration. The performance of FCV during one-lung ventilation (OLV) under intravascular normo- and hypovolaemia is currently unknown. In this explorative study, we hypothesised that OLV with FCV improves PaO2 and reduces mechanical power compared to volume-controlled ventilation (VCV). Sixteen juvenile pigs were randomly assigned to one of two groups: (1) intravascular normovolaemia (n = 8) and (2) intravascular hypovolaemia (n = 8). To mimic inflammation due to major thoracic surgery, a thoracotomy was performed, and 0.5 μg/kg/h lipopolysaccharides from Escherichia coli continuously administered intravenously. Animals were randomly assigned to OLV with one of two sequences (60 min per mode): (1) VCV-FCV or (2) FCV-VCV. Variables of gas exchange, haemodynamics and respiratory signals were collected 20, 40 and 60 min after initiation of OLV with each mechanical ventilation mode. The distribution of ventilation was determined using electrical impedance tomography (EIT).
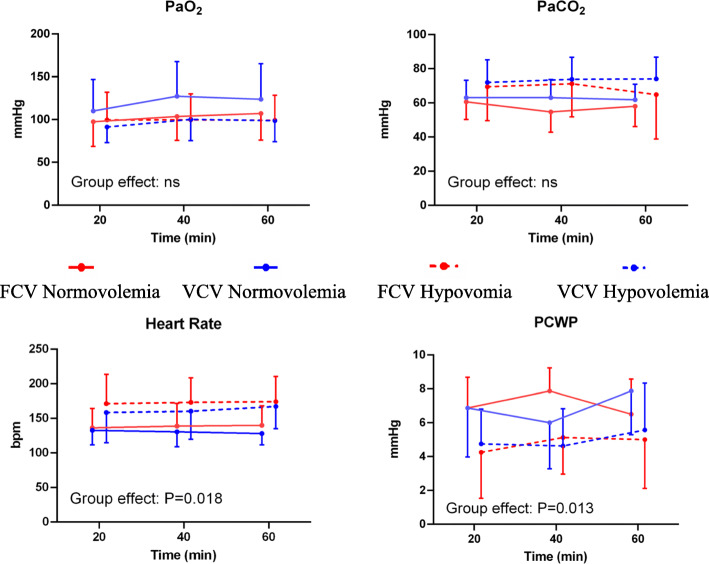
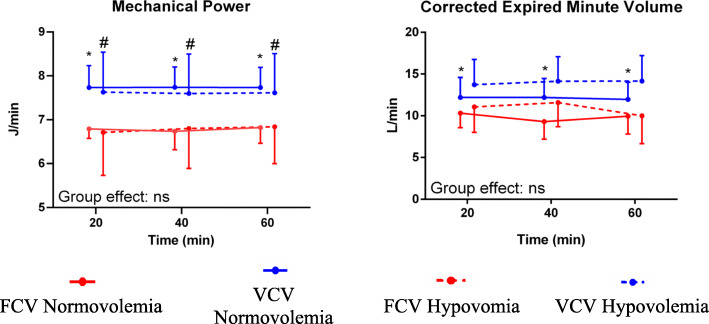
Results: Oxygenation did not differ significantly between modes (P = 0.881). In the normovolaemia group, the corrected expired minute volume (P = 0.022) and positive end-expiratory pressure (PEEP) were lower during FCV than VCV. The minute volume (P ≤ 0.001), respiratory rate (P ≤ 0.001), total PEEP (P ≤ 0.001), resistance of the respiratory system (P ≤ 0.001), mechanical power (P ≤ 0.001) and resistive mechanical power (P ≤ 0.001) were lower during FCV than VCV irrespective of the volaemia status. The distribution of ventilation did not differ between both ventilation modes (P = 0.103).
Conclusions: In a model of OLV in normo- and hypovolemic pigs, mechanical power was lower during FCV compared to VCV, without significant differences in oxygenation. Furthermore, the efficacy of ventilation was higher during FCV compared to VCV during normovolaemia.
Keywords: FCV; Hypoxemia; Intravascular hypovolaemia; Mechanical power; Normovolaemia; OLV; Resistive mechanical power; Thoracic surgery; VILI.
Conflict of interest statement
The authors declare that they have no competing interests
Figures
References
LinkOut - more resources
Full Text Sources
