

The effects of tidal volume size and driving pressure levels on pulmonary complement activation: an observational study in critically ill patients
- PMID: 33336309
- PMCID: PMC7746430
- DOI: 10.1186/s40635-020-00356-6
The effects of tidal volume size and driving pressure levels on pulmonary complement activation: an observational study in critically ill patients
Abstract
Background: Mechanical ventilation can induce or even worsen lung injury, at least in part via overdistension caused by too large volumes or too high pressures. The complement system has been suggested to play a causative role in ventilator-induced lung injury.
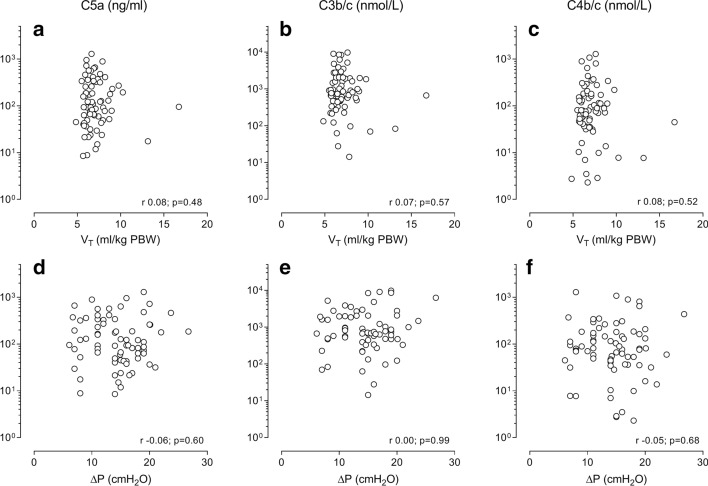
Aims and methods: This was a single-center prospective study investigating associations between pulmonary levels of complement activation products and two ventilator settings, tidal volume (VT) and driving pressure (ΔP), in critically ill patients under invasive ventilation. A miniature bronchoalveolar lavage (BAL) was performed for determination of pulmonary levels of C5a, C3b/c, and C4b/c. The primary endpoint was the correlation between BAL fluid (BALF) levels of C5a and VT and ΔP. Levels of complement activation products were also compared between patients with and without ARDS or with and without pneumonia.
Results: Seventy-two patients were included. Median time from start of invasive ventilation till BAL was 27 [19 to 34] hours. Median VT and ΔP before BAL were 6.7 [IQR 6.1 to 7.6] ml/kg predicted bodyweight (PBW) and 15 [IQR 11 to 18] cm H2O, respectively. BALF levels of C5a, C3b/c and C4b/c were neither different between patients with or without ARDS, nor between patients with or without pneumonia. BALF levels of C5a, and also C3b/c and C4b/c, did not correlate with VT and ΔP. Median BALF levels of C5a, C3b/c, and C4b/c, and the effects of VT and ΔP on those levels, were not different between patients with or without ARDS, and in patients with or without pneumonia.
Conclusion: In this cohort of critically ill patients under invasive ventilation, pulmonary levels of complement activation products were independent of the size of VT and the level of ΔP. The associations were not different for patients with ARDS or with pneumonia. Pulmonary complement activation does not seem to play a major role in VILI, and not even in lung injury per se, in critically ill patients under invasive ventilation.
Keywords: Bronchoalveolar lavage; C5a; Complement; Complement activation; Complement component 5; Critical care; Driving pressure; Intensive care; Mechanical ventilation; Tidal volume.
Conflict of interest statement
The authors declare that they have no competing interest.
Figures


References
-
- Serpa Neto A, et al. Lung-protective ventilation with low tidal volumes and the occurrence of pulmonary complications in patients without acute respiratory distress syndrome: a systematic review and individual patient data analysis. Crit Care Med. 2015;43(10):2155–2163. doi: 10.1097/CCM.0000000000001189. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
