

Effects of higher PEEP and recruitment manoeuvres on mortality in patients with ARDS: a systematic review, meta-analysis, meta-regression and trial sequential analysis of randomized controlled trials
- PMID: 33336325
- PMCID: PMC7746429
- DOI: 10.1186/s40635-020-00322-2
Effects of higher PEEP and recruitment manoeuvres on mortality in patients with ARDS: a systematic review, meta-analysis, meta-regression and trial sequential analysis of randomized controlled trials
Abstract
Purpose: In patients with acute respiratory distress syndrome (ARDS), lung recruitment could be maximised with the use of recruitment manoeuvres (RM) or applying a positive end-expiratory pressure (PEEP) higher than what is necessary to maintain minimal adequate oxygenation. We aimed to determine whether ventilation strategies using higher PEEP and/or RMs could decrease mortality in patients with ARDS.
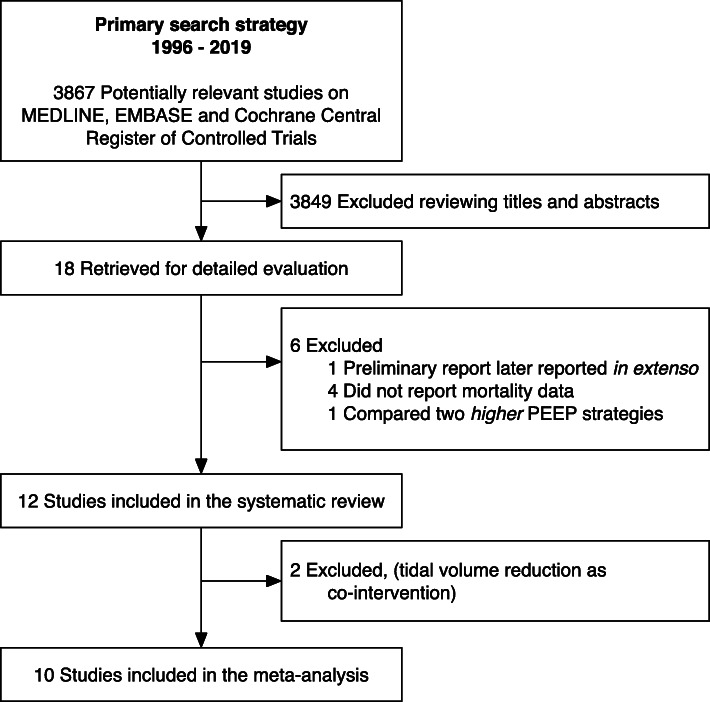
Methods: We searched MEDLINE, EMBASE and CENTRAL from 1996 to December 2019, included randomized controlled trials comparing ventilation with higher PEEP and/or RMs to strategies with lower PEEP and no RMs in patients with ARDS. We computed pooled estimates with a DerSimonian-Laird mixed-effects model, assessing mortality and incidence of barotrauma, population characteristics, physiologic variables and ventilator settings. We performed a trial sequential analysis (TSA) and a meta-regression.
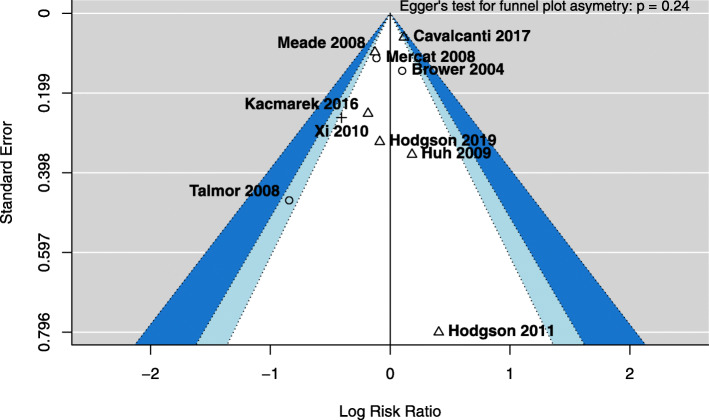
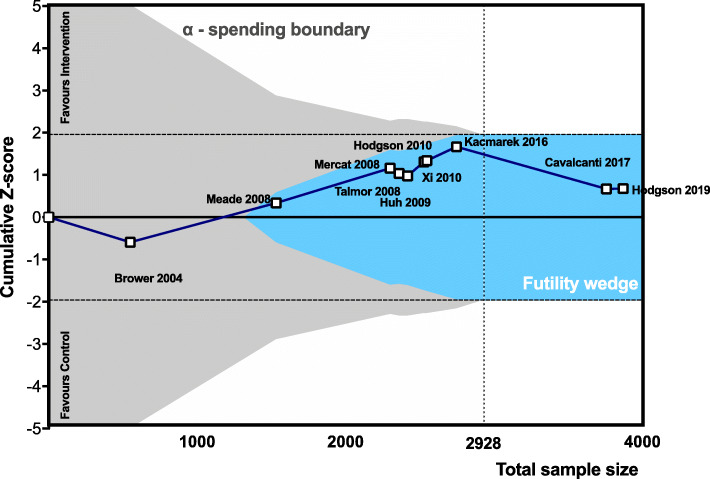
Results: Excluding two studies that used tidal volume (VT) reduction as co-intervention, we included 3870 patients from 10 trials using higher PEEP alone (n = 3), combined with RMs (n = 6) or RMs alone (n = 1). We did not observe differences in mortality (relative risk, RR 0.96, 95% confidence interval, CI [0.84-1.09], p = 0.50) nor in incidence of barotrauma (RR 1.22, 95% CI [0.93-1.61], p = 0.16). In the meta-regression, the PEEP difference between intervention and control group at day 1 and the use of RMs were not associated with increased risk of barotrauma. The TSA reached the required information size for mortality (n = 2928), and the z-line surpassed the futility boundary.
Conclusions: At low VT, the routine use of higher PEEP and/or RMs did not reduce mortality in unselected patients with ARDS.
Trial registration: PROSPERO CRD42017082035 .
Keywords: Acute respiratory distress syndrome; Mechanical ventilation; Positive end-expiratory pressure.
Conflict of interest statement
All authors declare that they have no conflict of interest.
Figures

References
-
- Cruz FF, Ball L, Rocco PRM, Pelosi P (2018) Ventilator-induced lung injury during controlled ventilation in patients with acute respiratory distress syndrome: less is probably better. Expert Rev Respir Med 1–12. 10.1080/17476348.2018.1457954 - PubMed
-
- Villar J, Kacmarek RM, Pérez-Méndez L, Aguirre-Jaime A. A high positive end-expiratory pressure, low tidal volume ventilatory strategy improves outcome in persistent acute respiratory distress syndrome: a randomized, controlled trial. Crit Care Med. 2006;34:1311–1318. doi: 10.1097/01.CCM.0000215598.84885.01. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
