

Veno-Arterial Extracorporeal Life Support in Heart Transplant and Ventricle Assist Device Centres. Meta-analysis
- PMID: 33337072
- PMCID: PMC8006654
- DOI: 10.1002/ehf2.13080
Veno-Arterial Extracorporeal Life Support in Heart Transplant and Ventricle Assist Device Centres. Meta-analysis
Abstract
Aims: Because reported mortality on veno-arterial (V-A) extracorporeal life support (ECLS) substantially varies between centres, the aim of the current analysis was to assess the outcomes between units performing heart transplantation and/or implanting ventricular assist device (HTx/VAD) vs. non-HTx/VAD units in patients undergoing V-A ECLS for cardiogenic shock.
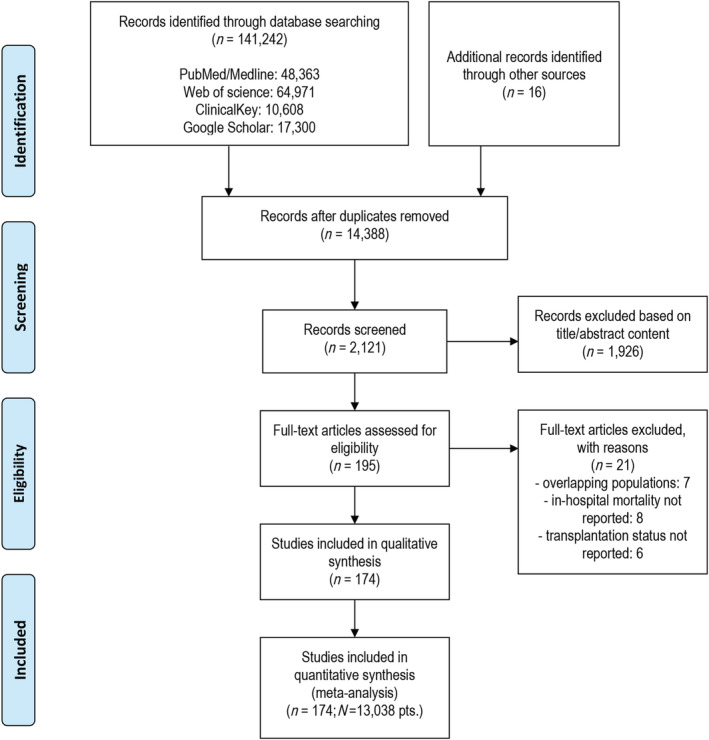
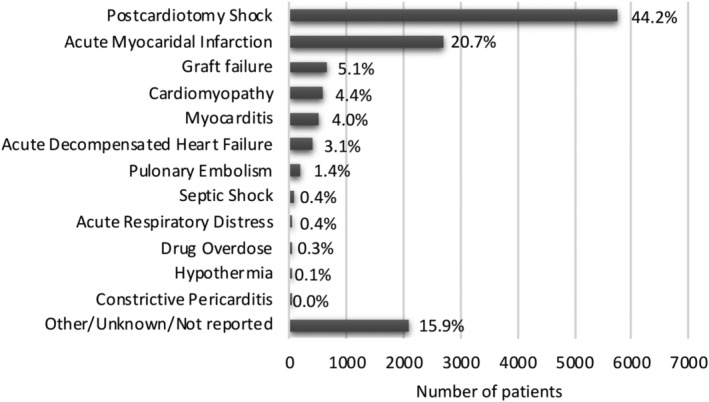
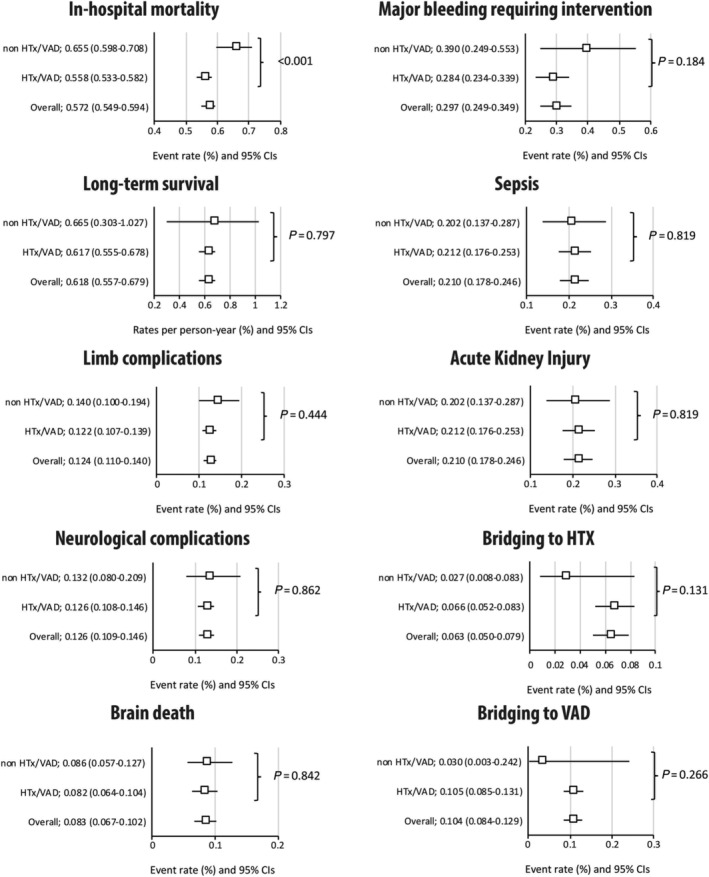
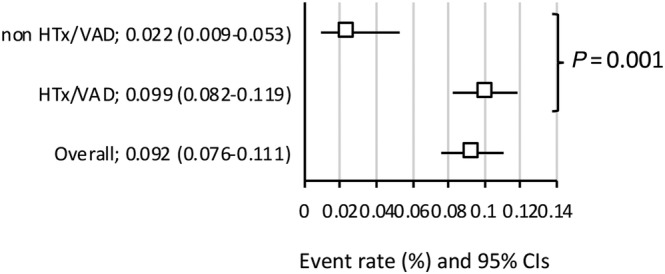
Methods and results: Systematic search according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses was performed using PubMed/MEDLINE databases until 30 November 2019. Articles reporting in-hospital/30-day mortality and centre's HTx/VAD status were included. In-hospital outcomes and long-term survival were analysed in subgroup meta-analysis. A total of 174 studies enrolling n = 13 308 patients were included with 20 series performed in non-HTx/VAD centres (1016 patients, 7.8%). Majority of patients underwent V-A ECLS for post-cardiotomy shock (44.2%) and acute myocardial infarction (20.7%). Estimated overall in-hospital mortality was 57.2% (54.9-59.4%). Mortality rates were higher in non-HTx/VAD [65.5% (59.8-70.8%)] as compared with HTx/VAD centres [55.8% (53.3-58.2%)], P < 0.001. Estimated late survival was 61.8% (55.7-67.9%) without differences between non-HTx/VAD and HTx/VAD centres: 66.5% (30.3-1.02%) vs. 61.7% (55.5-67.8%), respectively (P = 0.797). No differences were seen with respect to ECLS duration, limb complications, and reoperations for bleeding, kidney injury, and sepsis. Yet, weaning rates were higher in HTx/VAD vs. non-HTx/VAD centres: 58.7% (56.2-61.1%) vs. 48.9% (42.0-55.9%), P = 0.010. Estimated rate of bridge to heart transplant was 6.6% (5.2-8.3%) with numerical, yet not statistically significant, difference between non-HTx/VAD [2.7% (0.8-8.3%)] as compared with HTx/VAD [6.7% (5.3-8.6%)] (P = 0.131).
Conclusions: Survival after V-A ECLS differed according to centre's HTx/VAD status. Potentially different risk profiles of patients must be taken account for before definite conclusions are drawn.
Keywords: Acute heart failure; Cardiogenic shock; Extracorporeal life support; Meta-analysis.
© 2020 The Authors. ESC Heart Failure published by John Wiley & Sons Ltd on behalf of the European Society of Cardiology.
Conflict of interest statement
Dr Lorusso is consultant and conducts clinical trial for LivaNova (London, UK), is consultant for Medtronic (Minneapolis, MN), and an Advisory Board member of PulseCath (Arnhem, The Netherlands). The other authors have no conflicts of interest to disclose.
Figures
References
-
- Harjola VP, Lassus J, Sionis A, Køber L, Tarvasmäki T, Spinar J, Parissis J, Banaszewski M, Silva‐Cardoso J, Carubelli V, di Somma S, Tolppanen H, Zeymer U, Thiele H, Nieminen MS, Mebazaa A, CardShock Study Investigators , GREAT network . Clinical picture and risk prediction of short‐term mortality in cardiogenic shock. Eur J Heart Fail 2015; 17: 501–509. - PubMed
-
- Werdan K, Gielen S, Ebelt H, Hochman JS. Mechanical circulatory support in cardiogenic shock. Eur Heart J 2014; 35: 156–167. - PubMed
-
- Lorusso R, Raffa GM, Alenizy K, Sluijpers N, Makhoul M, Brodie D, McMullan M, Wang IW, Meani P, MacLaren G, Kowalewski M, Dalton H, Barbaro R, Hou X, Cavarocchi N, Chen YS, Thiagarajan R, Alexander P, Alsoufi B, Bermudez CA, Shah AS, Haft J, D'Alessandro DA, Boeken U, Whitman GJR. Structured review of post‐cardiotomy extracorporeal membrane oxygenation: part 1—adult patients. J Heart Lung Transplant 2019; 38: 1125–1143. - PMC - PubMed
-
- Whitman GJ. Extracorporeal membrane oxygenation for the treatment of postcardiotomy shock. J Thorac Cardiovasc Surg 2017; 153: 95–101. - PubMed
-
- Lorusso R, Gelsomino S, Parise O, Mendiratta P, Prodhan P, Rycus P, MacLaren G, Brogan TV, Chen YS, Maessen J, Hou X, Thiagarajan RR. Venoarterial extracorporeal membrane oxygenation for refractory cardiogenic shock in elderly patients: trends in application and outcome from the extracorporeal life support organization (elso) registry. Ann Thorac Surg 2017; 104: 62–69. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
