

Current View of Diagnosing Small Fiber Neuropathy
- PMID: 33337383
- PMCID: PMC8075405
- DOI: 10.3233/JND-200490
Current View of Diagnosing Small Fiber Neuropathy
Abstract
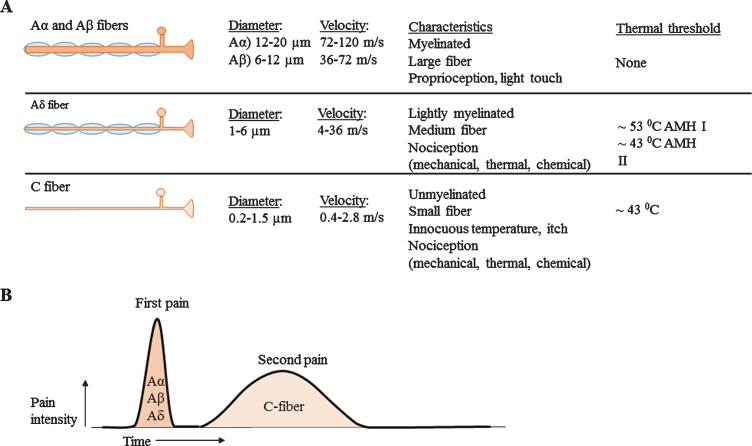
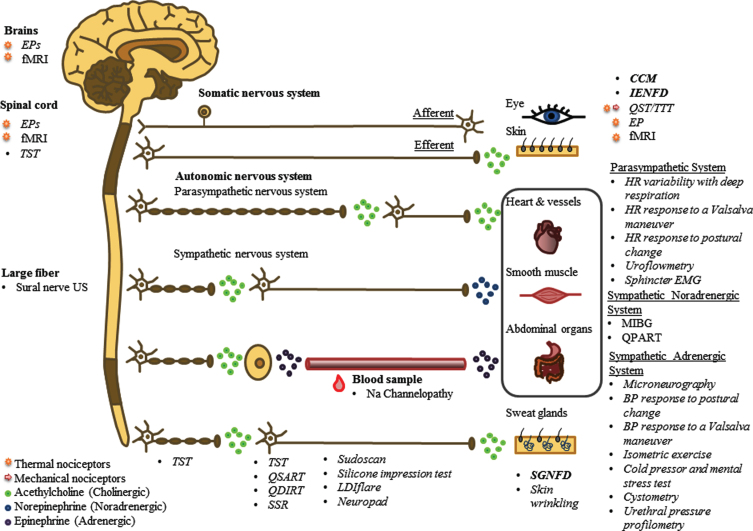
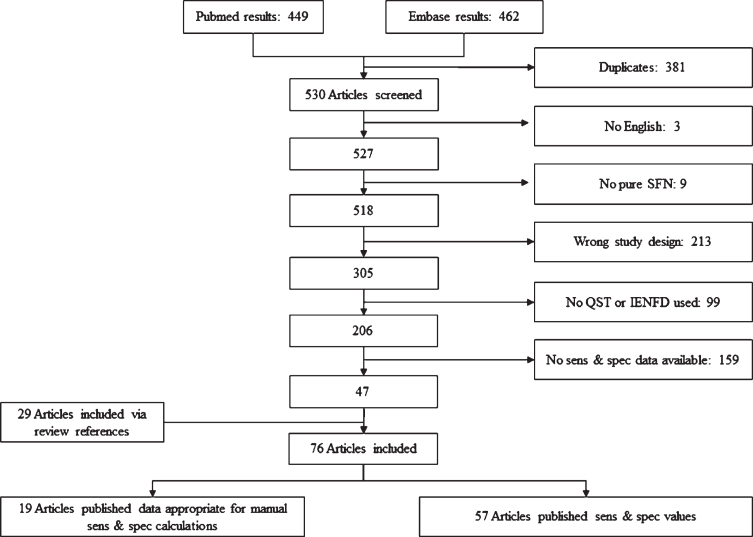
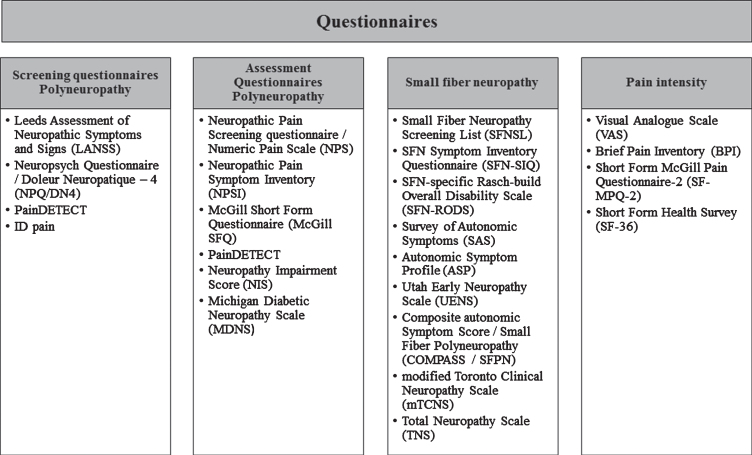
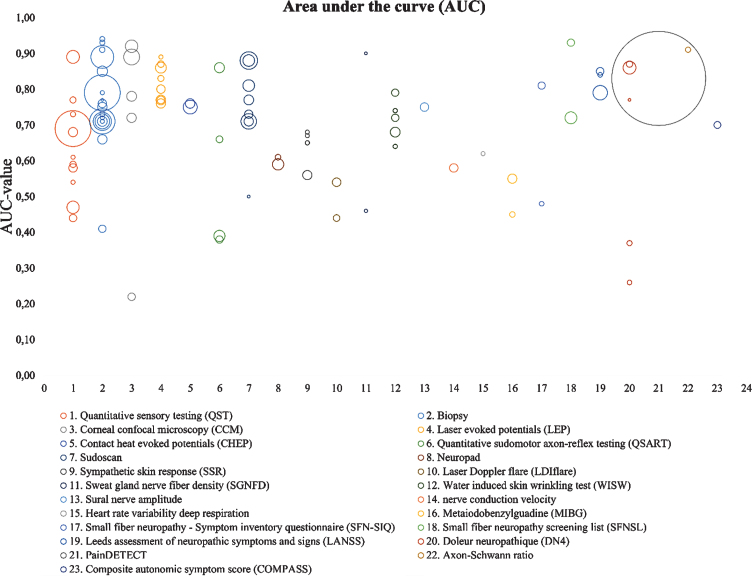
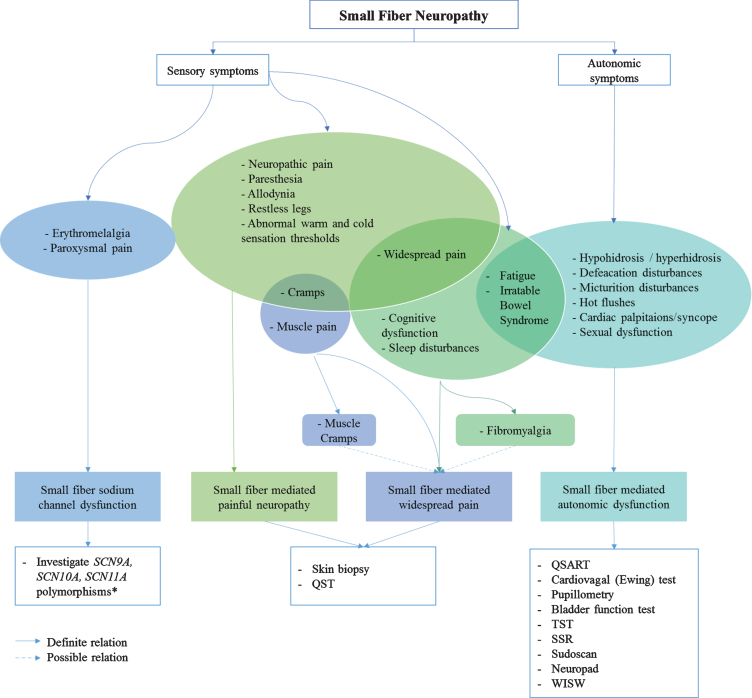
Small fiber neuropathy (SFN) is a disorder of the small myelinated Aδ-fibers and unmyelinated C-fibers [5, 6]. SFN might affect small sensory fibers, autonomic fibers or both, resulting in sensory changes, autonomic dysfunction or combined symptoms [7]. As a consequence, the symptoms are potentially numerous and have a large impact on quality of life [8]. Since diagnostic methods for SFN are numerous and its pathophysiology complex, this extensive review focusses on categorizing all aspects of SFN as disease and its diagnosis. In this review, sensitivity in combination with specificity of different diagnostic methods are described using the areas under the curve. In the end, a diagnostic work-flow is suggested based on different phenotypes of SFN.
Keywords: Autonomic dysfunction; diagnostic accuracy; nerve fiber density; small fiber neuropathy.
Conflict of interest statement
The authors declare no competing financial interests
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
